Head And Neck Images: Key Learning Points For Residency
Aug 27, 2025
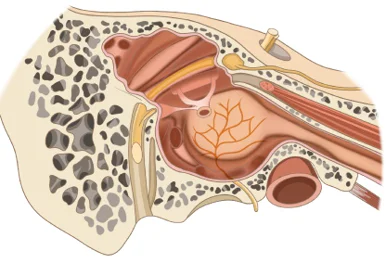
Facial Nerve Transposition in Ear Canal Wall Down
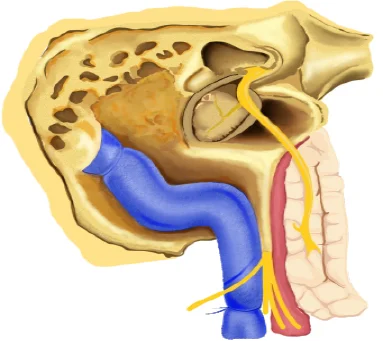
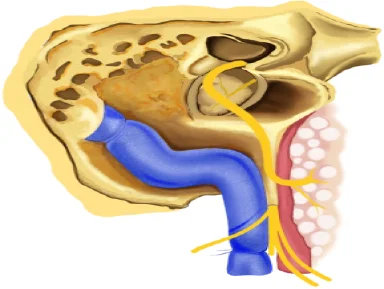
In order to be able to mobilize the facial nerve more extensively, atticomastoidectomy should be extended to subtotal petrosectomy. This involves the removal of the skin of the external auditory
meatus along with the tympanic membrane, the malleus and incus, drilling away the posterior canal wall and extensive exenteration of pneumatic cells. As a result, the facial nerve can be uncovered not only in its mastoid segment but also in its tympanic part. The nerve can be rerouted anteriorly after the mobilization of the intraparotid facial nerve. The hinge point may be located at the second genu, but wider exposure is achieved when the nerve is displaced anteriorly with the hinge point at the first genu.
Petrous Apex Lesions
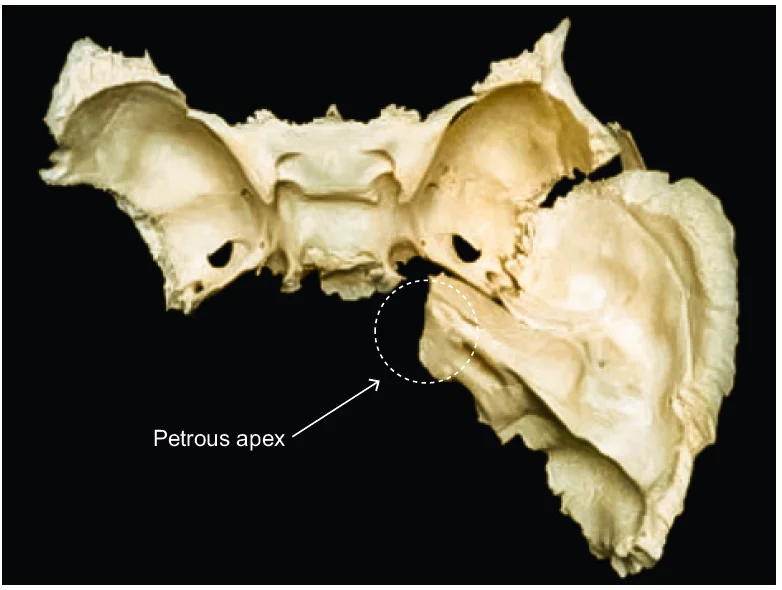
The petrous apex is a complex bone, a part of the temporal bone. The petrous bone is a leaf-shaped structure located between the greater wing of the sphenoid bone and the occipital bone. Its apex is situated near the clivus of the sphenoid bone, where the clivus serves as the medial boundary, the greater wing of the sphenoid bone as the anterior boundary, and the
occipital bone as the posterior boundary. This bone exhibits both superior and posterior surfaces. The superior part forms the floor of the middle cranial fossa, while the posterior surface marks the anterior aspect of the cerebellopontine angle.
Chorda Tympani
Terminal branch of nervus intermedius. The Chorda tympani nerve goes through pars flaccida and from posterior canaliculus, it passes between the long process of incus and the malleus, and exits from the anterior canaliculus. This point is also called the Canal of Hugier.
Nerve to Stapedius
It arises from neurons outside the nucleus. This may explain the normal function of the stapedius muscle in congenital facial palsy and the alterations in the stapedial reflexes in brainstem lesions.
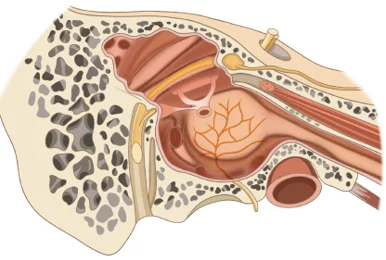
Neuropathophysiology of the Facial Nerve
Whenever there is facial nerve palsy, it is crucial to know if there is neuropraxia, axonotmesis, or neurotmesis. In this, there are central axons covered with myelin sheath. Over the myelin sheath covering, there is another layer, which is endoneurium. Over this, there is another layer named Perineurium and the final layer Epineurium.

Electroneuronography
Supramaximal stimulus is delivered to the facial nerve trunk as it exits the stylomastoid foramen. The response of the paralyzed side is compared with the normal one, which serves as a control, and the percent of degenerated fibers are calculated. Example: if the patient is given Supramaximal stimulus on the left (normal) and right side (paralyzed side). If the contraction was 10% on the right side while the left is 100%. Such reduction is significant.
Moebius Syndrome

There is a congenital facial weakness with impairment of ocular abduction. Dysfunction of other cranial nerves - III, IV, IX, X, XII. Skeletal abnormalities: (Oro-facial, limb malformations). Pathogenesis is usually genetic causes vs ischemic causes.
Surface Anatomy of the Neck
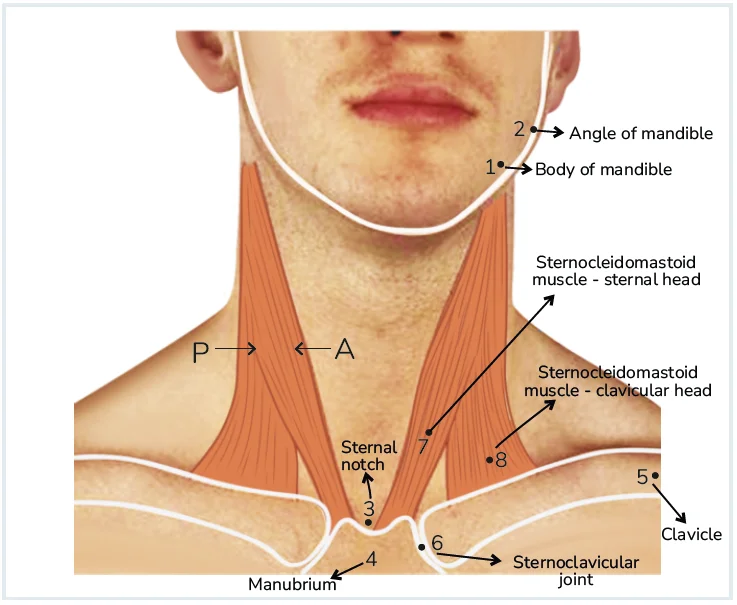
The neck extends from the mandible superiorly and inferiorly from the clavicle and sterno clavicular joint. The sternocleidomastoid muscle divides the neck into two triangles. Medial to it is an anterior triangle, and posterior to it is a posterior triangle. The superior border of the neck is defined by the mandible with the deep limits of the floor of the mouth anteriorly and the skull base posteriorly. The upper aspects of the first rib and the first thoracic vertebrae form the inferior limit of the neck.
Sternocleidomastoid Muscle
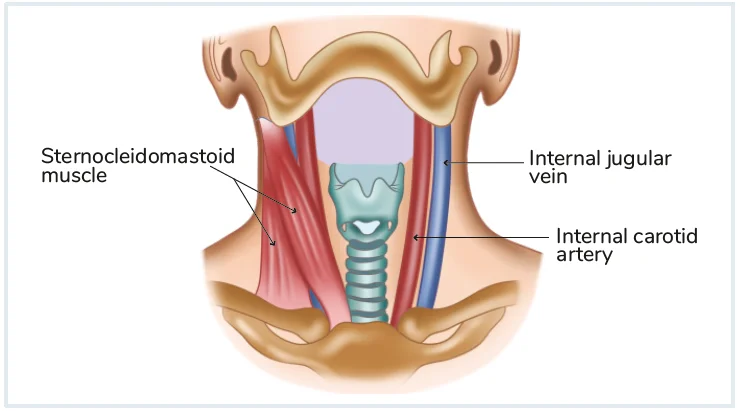
It is a muscle that comes from the sternum and clavicle and goes to the mastoid tip superiorly.
The sternocleidomastoid divides the neck into anterior and posterior triangles. The carotid sheath runs deep to the sternocleidomastoid muscle. The carotid sheath contains the internal carotid artery, the internal jugular vein, and the 9th, 10th, and 11th nerve. The bulk of the muscle provides a degree of protection to the major vessels from penetrating neck injuries. The lymph nodes of the jugular chains are located deeper into the muscles.
Submandibular Triangle
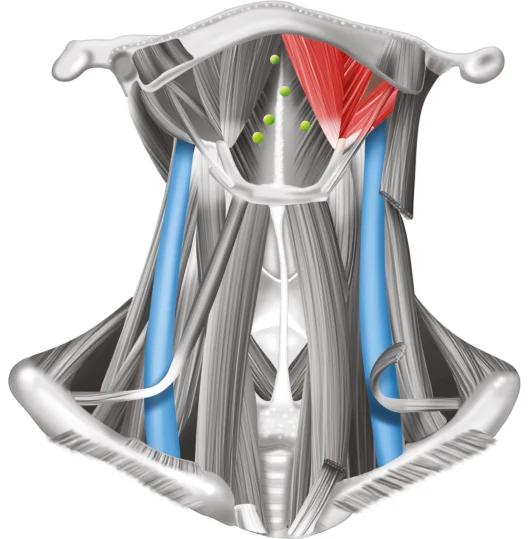
It is also known as digastric triangle. It is bounded by anterior and posterior bellies of digastric and body of mandible. Floor is formed by mylohyoid and hyoglossus muscles. It comprises the facial artery and vein, marginal mandibular branch of the facial nerve, submandibular salivary gland, submandibular group of lymph nodes (level Ib).
Lymphangiomas
These are the degenerative lesions arising from lymphatics and are classified as Simple lymphangiomas, Cavernous lymphangiomas, and Cystic hygromas.
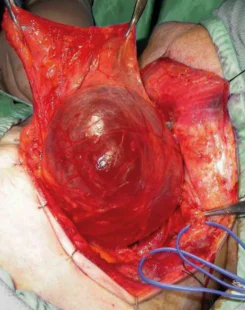
Thyroglossal Duct Cysts

Thyroglossal duct cysts are the most common upper neck midline lesion. They can present as a mass or lump at any level between the foramen caecum and the upper mediastinum, with the
majority presenting about the level of the hyoid bone.Thyroglossal duct carcinoma, although rare, may be identified by a pathologist in a thyroglossal duct cyst.
Tuberculous Adenitis

Increased incidence is due to the rising incidence of immunodeficiency through HIV infections or intravenous drug abuse. Pulmonary tuberculosis is the most common manifestation but the extrapulmonary disease is also increasing in incidence with tuberculosis adenitis, historically named scrofula, being the most common.
Ear Foreign Bodies
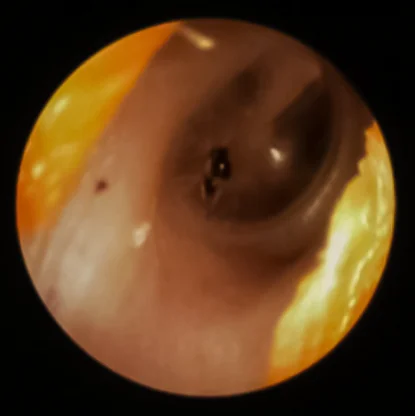
The above picture shows an inert foreign body sitting upon the tympanic membrane. It can be left as it is and will migrate out by itself. If the patient has symptoms, microsuction can be performed. Typically, a local anesthesia drop or spray is applied to anesthetize the tympanic membrane, and then the foreign body is removed. It is better not to use a hook over the tympanic membrane, as it may accidentally cause tympanic membrane perforation.
Pembertons Sign
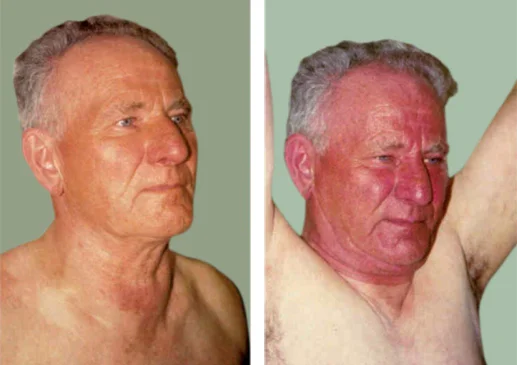
The Pemberton's sign, which involves lifting the arms along the ears on the side of the face for one minute, can lead to congestion of the face, redness of the face, cyanosis, or respiratory distress, providing further diagnostic information.
Antero Lateral Neck Dissection
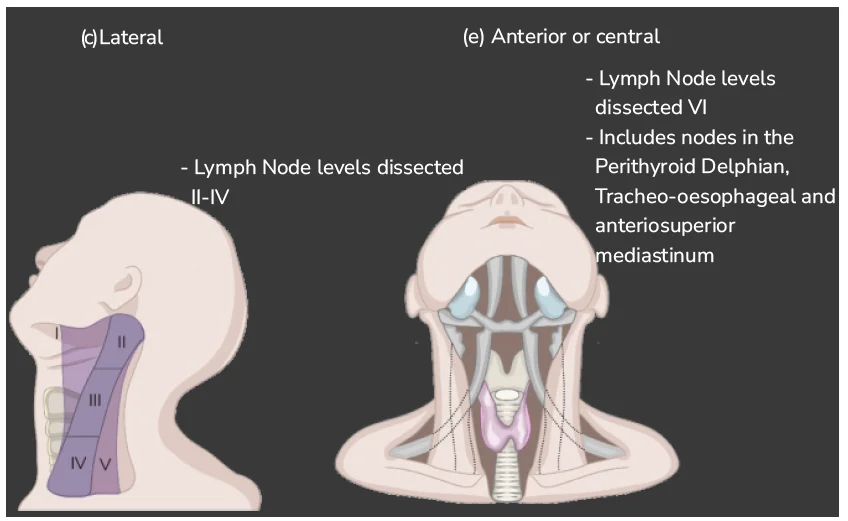
In lateral neck dissection there is removal of level 1,2,3,4 and 5. In anterior neck dissection, there is a removal of level VI lymph nodes, and along with that, perithyroid, delphian, tracheo-esophageal, and anterosuperior mediastinum nodes are removed. So it is anterolateral neck dissection.
Masseter Transfer Procedure
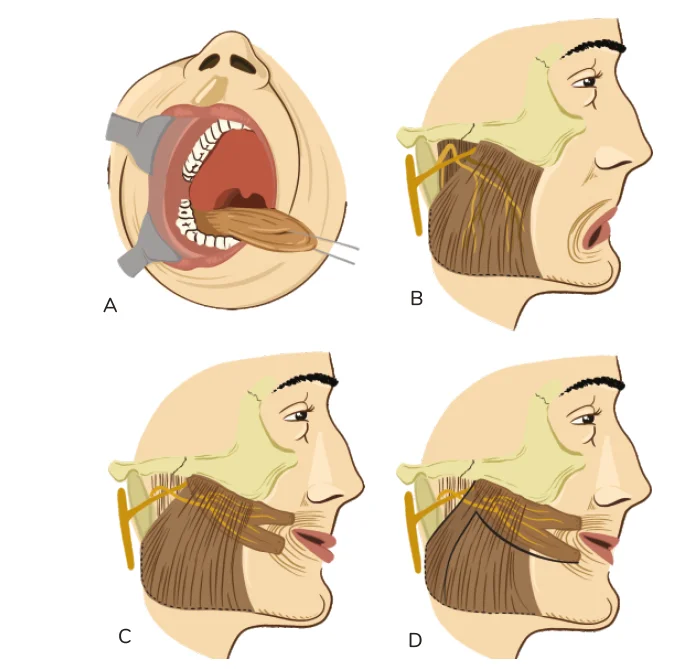
Intraoral approach to masseter. The procedure is more difficult when performed in this manner; an external approach is preferred. There needs to be correct incisions in the muscle and periosteum. Periosteum must be incorporated in the lower portion of the muscle flap to leave the tissue secure for suturing to the lip region. Entire muscle rather than only anterior elements, is transpired, so that the masseteric nerve supply is transferred intact with muscle belly.
Hope you found this blog helpful for your Basic Sciences Preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.
Propel your ENT Residency Preparation! Access conceptual video lectures, QBank, Mock Tests, and premium study resources on the PrepLadder App. Download it today!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!