Transoral Robotic Surgery (TORS) in ENT
Aug 27, 2025
Transoral Robotic Surgery
Benign Tumors of the nasopharynx and parapharyngeal space are curated by Robotic surgery.
Indications are evolving in Transoral robotic surgery.
Contraindications:
Malignant tumors with lateral extension, significant dural invasion, and intracranial extension.
Malignant lesions that require a degree of lateral access, those that extend into the lateral parapharyngeal space, cavernous sinus, posterior infratemporal fossa, and posterior peritubal space.
Principles of the procedure
Transoral robotic surgery (TORS) is the most recent surgical modality that has the potential to further improve surgery in this anatomic region. The range of wrist-mediated instrument mobility combined with the 3D visualization of the operating field opens up a new paradigm in our specialty. The upcoming introduction of the single-port vision of the DaVinci system offers hope in the management of midline lesions. Current limitations of the technology are related to the lack of haptic feedback and the lack of instrumentation to remove and remodel bone effectively.
Advantages of TORS:
It is a direct approach, unparalleled instrument dexterity, and high mobility. It has an HD 3D visualization of the operating field.
Limitations and Drawbacks:
It has high set-up costs, utility and indications to be defined. Current case series report on confined lesions of the posterior nasopharyngeal wall and benign tumors of the parapharyngeal
Space. Clinical outcomes data is in the evolving stage as of now.
Transoral and Transpalatine Approaches
Malignant tumors of the posterior nasopharyngeal wall that are no larger than 2 cm. Access to tumor extension into the clivus and craniocervical junction
Contraindications involve:
Malignant nasopharyngeal tumors more than 2 cm in size. Tumors with significant dural invasion and intracranial extension. Lesions that require a degree of lateral access, those that
extend into the parapharyngeal space, cavernous sinus, infratemporal fossa, and peritubal space.

Procedure of Transoral Robotic Surgery (TORS) in ENT
The patient is placed in the supine position with their head extended as much as possible.
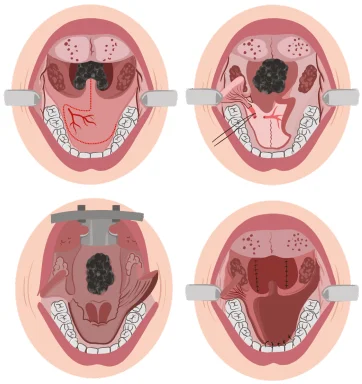
A preliminary tracheostomy is established so that an unobstructed view of the oropharynx is obtained and to secure the airway post-operatively, as most patients will develop significant lingual and oropharyngeal edema. If there is a possibility of CSF the, Lumbar CSF drainage is inserted if the dura is to be opened. After insertion of the mouth gag and retraction of the oral cavity, the soft and hard palate is infiltrated with 1: 200000 adrenaline. The soft palate is split to one side of the midline. The hard palate mucosa is incised along the ipsilateral junction of the hard and soft palate within 5 mm of the maxillary dentition.
The mucosal incision is extended along the palatal aspect of the alveolar ridge up to the level of the first molar and then taken in an arc across the palate to the opposite side. A mucoperiosteal flap is elevated exposing the bony hard palate. The greater palatine neurovascular bundle is coagulated and divided.
Exposure of the nasopharynx is increased by dissection of the muscular insertions of the soft palate from the hard palate. Great care must be taken to maintain the integrity of the remaining greater palatine vascular pedicle while doing this. A self-retaining retractor is then inserted to keep the 2 halves of the soft palate out of the field.
Dissection through the posterior nasopharyngeal wall gives access to the lower clivus. If the lesion extends towards the sphenoid floor or the upper clivus the operative field must be enlarged. In some cases this can be achieved by removal of some palatal vomerine bone. In others, it will be necessary to perform a Le Fort I. Osteotomy and then split the palate in the midline, displacing each maxilla laterally.
This latter approach, known as an open-door maxillectomy, can offer unrivaled exposure of the entire clivus and craniocervical junction. A suitable mucosal flap is raised and hinged either laterally or inferiorly. The length of this flap varies according to the extent of the lesion being removed. The larger the flap, the better the chance of being able to approximate it at the end of the procedure.
If the lesion is submucosal, it is usually unnecessary to split the prevertebral fascia. But if it is necessary to access the clivus the prevertebral fascia and muscles have to be opened, and this is best undertaken in the midline. The most helpful anatomical landmark is the anterior arch of the atlas, which is easily palpable. Apart from very small dural tears or defects that can be plugged with muscle, primary watertight closure is virtually impossible; however, the advent of new dural sealing materials might alter this condition.
The dead space created by tumor resection can be filled with autograft soft tissue secured in place by fibrin glue. It is best covered by pedicled local mucosal or mucoperichondrial flaps raised from the nasal septum and rotated into place. As much as possible prevertebral fascia, musculature, and pharyngeal mucosa are reappoximated. The soft palate is readapted, preferably through a three layered closure, in this way, the chance of an oro-nasal fistula developing is minimised.
Advantages:
It is a simple technique, gives us a direct approach, and it is extendable through the LeFort I-palatal split approach.
Limitations and drawbacks includes:
- Requirement for tracheostomy
- Narrow working field and long working distance
- Possible palatal dehiscence and oronasal fistula as a late complication in 30-40%
- Patients with trismus or impaired jaw opening require a trans mandibular approach
- No access laterally to the parapharyngeal and infratemporal spaces
- There is a risk of meningitis due to wound contamination.
Hope you found this blog helpful for your Basic Sciences Preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.
Propel your ENT Residency Preparation! Access conceptual video lectures, QBank, Mock Tests, and premium study resources on the PrepLadder App. Download it today!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Transoral Robotic Surgery
Contraindications:
Principles of the procedure
Advantages of TORS:
Limitations and Drawbacks:
Transoral and Transpalatine Approaches
Contraindications involve:
Procedure of Transoral Robotic Surgery (TORS) in ENT
Advantages:
Limitations and drawbacks includes: