High-Yield Anatomy Topics That Frequently Repeat in FMGE
Jun 19, 2026
Anatomy has been recognised as the structural foundation of medical education. As per the FMGE pattern, it has a constant and significant weightage of around 17 marks. But this subject is worth much more than just 17 marks.
This is because Anatomy acts as the foundational gateway through which you get into the most difficult clinical subjects, such as General Surgery, Orthopaedics, Radiodiagnosis (radiology), and Obstetrics & Gynaecology.
When you are nearing the time of the examination, and you try to remember each and every muscle insertion or arterial branch from an atlas of 1,000 pages, then this exercise becomes futile. The examination follows the principle of 80/20, where 80% of all questions come from 20% of concepts.
Mastering these high-yield topics of Anatomy and using your active visual recall will help you score these vital marks easily. This article gives you an overview of the most important high-yield topics that should be mastered in each of the anatomical areas.

1. Upper Limb: Plexuses & Clinical Nerve Lesions
The upper limb always ranks among the most favoured parts by FMGE examiners. Questions from this section deal with complicated nerve injuries that occur as a consequence of particular fractures.
Anatomy of the Brachial Plexus
Knowledge of the brachial plexus is absolutely necessary; it has to include knowledge about its complete structure, from roots to terminal branches. Some typical cases are listed below:
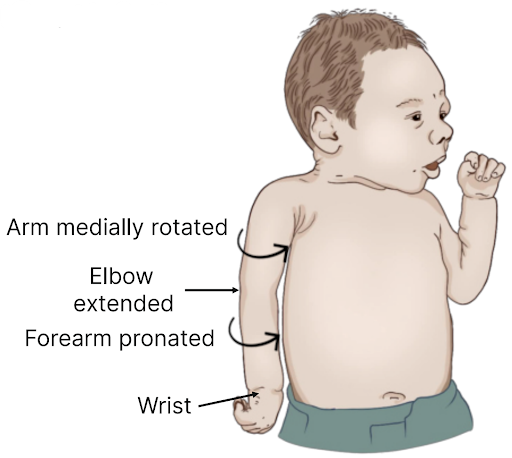
- Erb’s Palsy (Upper Trunk Injury): Caused by an abnormal increase in the angle between the head and shoulder (such as during birth trauma or falling on the shoulder), affecting roots C5 and C6. This condition presents with a 'Policeman's Tip' hand or "Waiter's Tip" hand because of loss of abduction, lateral rotation, and flexion at the elbow.
- Klumpke’s Palsy (Lower Trunk Injury): Caused by hyper-abduction of the arm (e.g., clutching an object while falling from a height). It involves roots C8 and T1, leading to a dramatic loss of intrinsic hand muscle function, resulting in a true claw hand presentation.

Download the Academic PDF for FREE and Boost your Exam Prep
Upper Limb Nerve Deformities & Fracture Correlations
Use this quick-reference matrix to link a specific skeletal fracture site to its corresponding nerve injury and clinical presentation:
| Injured Nerve | Specific Fracture / Injury Site | Resulting Deformity & Clinical Signs | Key Muscle / Functional Deficit |
| Radial Nerve | Mid-shaft Humeral Fracture / Spiral Groove | Wrist Drop | Loss of extension in the wrist and fingers |
| Median Nerve | Supracondylar Humeral Fracture / Carpal Tunnel | Ape Thumb Deformity / Hand of Benediction | Loss of thumb opposition and lateral lumbrical flexion |
| Ulnar Nerve | Medial Epicondyle Fracture | Ulnar Claw Hand | Flexion at interphalangeal joints of 4th & 5th digits |
| Axillary Nerve | Surgical Neck of Humerus / Shoulder Dislocation | Regimental Badge Sign / Flat Shoulder | Paralysis of the Deltoid muscle (loss of abduction) |
2. Lower Limb: Nerve Coordinates, Gates & Clinical Deformities
Lower limb anatomy balances the upper limb section by testing major plexuses, joint instabilities, and gait abnormalities related to compartment nerve supplies.
- Femoral Nerve (L2–L4): Supplies the anterior compartment of the thigh (including the Quadriceps femoris). Injury leads to a loss of knee extension and wasting of the anterior thigh, often seen after deep groin penetrations or pelvic fractures.
- Obturator Nerve (L2–L4): Passes through the obturator foramen to supply the medial adductor compartment of the thigh. Injury causes severe weakness in thigh adduction.
- Sciatic Nerve & The Popliteal Fossa: The largest nerve in the body, vulnerable during posterior dislocations of the hip joint. It splits into the tibial and common peroneal nerves at the apex of the popliteal fossa.
Also Read: Best Subject-Wise Revision Order for FMGE June 2026
Lower Limb Peripheral Nerve Summary
Nerve Root Value Main Muscles Supplied Clinical Injury Presentation Common Peroneal Nerve L4–S2 Anterior & Lateral compartments of the leg Foot Drop (loss of dorsiflexion/eversion); High-steppage gait Tibial Nerve L4–S3 Posterior compartment of the leg (Calf muscles) Loss of plantarflexion; Inability to stand on tiptoes Femoral Nerve L2–L4 Iliopsoas, Pectineus, Quadriceps femoris Loss of knee extension; Diminished patellar reflex
3. Neuroanatomy: The Circle of Willis, Cranial Nerves & Dural Sinuses
Neuroanatomy questions are highly visual and offer excellent scoring opportunities once the major pathways and structural relationships are mapped.
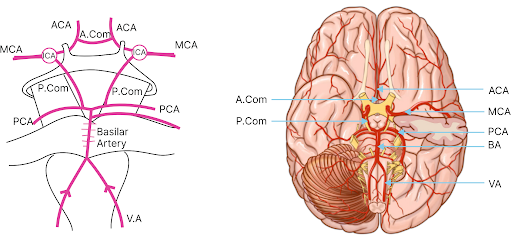
Circle of Willis and Cerebrovascular Anomalies
This arterial ring, located at the base of the brain, is frequently tested via radiological layouts and schematic diagrams. You must master the contributions of the internal carotid arteries and the vertebrobasilar system:
- Anterior Communicating Artery: Common site for berry aneurysms, which can lead to bitemporal hemianopia due to compression of the optic chiasm.
- Middle Cerebral Artery (MCA): The most common site for ischemic strokes. Obstruction results in contralateral hemiplegia affecting the face and upper limb more than the lower limb.
Cranial Nerves & Cranial Foramina Lockouts
The exam frequently builds questions asking cranial nerve exits through specific skull base openings:
| Skull Base Opening (Foramen) | Transmitted Cranial Nerve(s) & Structures |
| Cribriform Plate | CN I (Olfactory nerve) |
| Optic Canal | CN II (Optic nerve) + Ophthalmic Artery |
| Superior Orbital Fissure (SOF) | CN III, CN IV, CN V1 (Ophthalmic Trigeminal), CN VI |
| Foramen Rotundum | CN V2 (Maxillary Trigeminal) |
| Foramen Ovale | CN V3 (Mandibular Trigeminal) |
| Internal Acoustic Meatus | CN VII (Facial nerve) + CN VIII (Vestibulocochlear nerve) |
| Jugular Foramen | CN IX, CN X (Vagus nerve), CN XI |
| Hypoglossal Canal | CN XII (Hypoglossal nerve) |
Also Read: Most Volatile Subjects in FMGE '26 & How to Retain Them Better
The Cavernous Sinus Anatomy
Study carefully the anatomical borders and localisation of structures passing through the cavernous sinus:
- Running through the centre: The Internal Carotid Artery and CN VI (Abducens nerve). Because it sits freely inside the sinus, CN VI is the first nerve involved in Cavernous Sinus Thrombosis, characterised by a loss of abduction of the eye.
- Embedded in the lateral wall (Top to Bottom): CN III (Oculomotor), CN IV (Trochlear), V1 (Ophthalmic), and V2 (Maxillary).
4. Head and Neck: Triangles, Glands and Key Spaces
The complicated spatial relationships within the head and neck make this area a common subject of multidisciplinary, high-yield MCQs.
- Triangles of the Neck: Concentrate particularly on the boundaries and core contents of the Carotid Triangle (containing the carotid bifurcation, internal jugular vein, and vagus nerve) and the Submandibular Triangle
- The Thyroid Gland Relations: Essential for integrating general surgery. Understand in detail the relationship between the superior thyroid artery and the external laryngeal nerve and between the inferior thyroid artery and the recurrent laryngeal nerve. Accidental ligation during surgery leads to characteristic vocal changes.
- The Parotid Gland: Focus on the structures passing through it from superficial to deep: the Facial Nerve (CN VII), Retromandibular Vein, and External Carotid Artery.
5. Thorax: Coronary Circulation & Diaphragmatic Levels
Thorax questions are very practical and often integrated directly with emergency medicine interventions and radiological imaging.
Blood Supply of the Heart
Learn about coronary artery distribution to become an expert at combining Anatomy with ECG reading in General Medicine courses:
- Left Anterior Descending (LAD) Artery: The "Widow-maker" artery, supplying the anterior surface of the left ventricle and two-thirds of the interventricular septum. Occlusion results in an anterior wall myocardial infarction.
- Right Coronary Artery (RCA): Supplies the sinoatrial (SA) node and the atrioventricular (AV) node, as well as the Inferior & Posterior Left Ventricle. Occlusion leads to inferior wall MI and severe bradycardia.
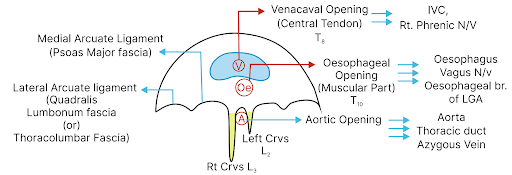
The Diaphragm Openings & Associated Vertebral Levels
Understand the exact major openings of the thoracoabdominal diaphragm along with the respective vertebrae milestones:
| Diaphragmatic Opening | Vertebral Level | Key Transmitted Structures |
| Vena Cava Opening | T8 | Inferior Vena Cava (IVC), Right Phrenic Nerve branches |
| Esophageal Opening | T10 | Esophagus, Anterior & Posterior Vagal Trunks |
| Aortic Opening | T12 | Aorta, Thoracic Duct, Azygos Vein |
6. Abdomen: Hernias, Portocaval Anastomosis & Core Vessels
Questions on abdominal structures have substantial overlap with General Surgery topics.
Inguinal Canal Anatomy & Hernia Differentiation
It is important to learn the anatomical landmarks differentiating direct from indirect inguinal hernia relative to the inferior epigastric vessels:
- Indirect Inguinal Hernia: The hernia sac enters the deep inguinal ring lateral to the inferior epigastric vessels and descends the full length of the inguinal canal due to a congenital patent processus vaginalis.
- Direct Inguinal Hernia: The hernia sac bulges directly through the posterior wall of the inguinal canal medial to the inferior epigastric vessels, directly through Hesselbach's Triangle because of an acquired weakness.
Portocaval Anastomosis & Portal Hypertension
Remember the formation of the portal vein from the confluence of the superior mesenteric vein and the splenic vein. Learn the key clinical sites of portocaval anastomosis to solve clinical cases of portal hypertension:
| Anatomical Site | Portal Component | Systemic Component | Clinical Presentation (Varices) |
| Lower end of Esophagus | Left Gastric Vein | Esophageal branch of Azygos | Esophageal Varices (Hematemesis) |
| Around the Umbilicus | Paraumbilical Veins | Superficial Epigastric Vein | Caput Medusae |
| Lower end of the rectum | Superior Rectal Vein | Middle & Inferior Rectal Veins | Internal Hemorrhoids |
7. Pelvis and Perineum: Spaces, Ligaments & Urinary Contours
The pelvis section forms the structural foundation for scoring well in Obstetrics & Gynaecology and Urology.
- The Ureteric Pathway: Very important from the surgical safety perspective. The ureter runs inferior to the uterine artery ("water under the bridge"). This is a high-yield zone that can be injured during a hysterectomy.
- Perineal Pouches: Learn the boundaries separating the deep and superficial perineal pouches. Know what structures lie within them (e.g., bulbourethral glands, internal pudendal vessels, and roots of external genitalia).
- Pelvic Floor & Diaphragm: Focus on the Levator ani muscle complex (Puborectalis, Pubococcygeus, and Iliococcygeus). Weakness in this area will lead directly to uterine or rectal prolapse clinical case scenarios.

8. Embryology & General Histology
The topics of embryology, joint classifications, and histology are very predictable and offer good scores.
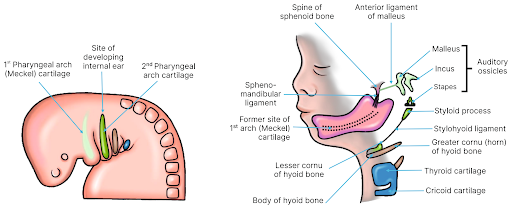
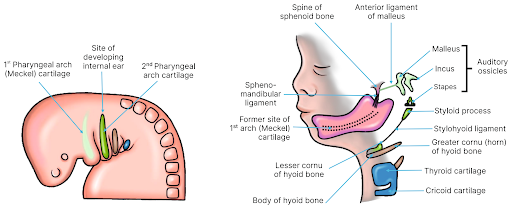
Pharyngeal (Branchial) Arch Derivatives
Learn the muscle, bone, and nerve derivatives for each pharyngeal arch because this table is a favourite for NBE exams:
| Branchial Arch | Associated Cranial Nerve | Core Skeletal/Cartilage Derivatives | Key Muscle Derivatives |
| 1st Arch (Mandibular) | CN V (Trigeminal nerve) | Malleus, Incus, Mandible | Muscles of mastication, Tensor tympani |
| 2nd Arch (Hyoid) | CN VII (Facial nerve) | Stapes, Styloid process, Lesser cornu of the hyoid | Muscles of facial expression, Stapedius |
| 3rd Arch | CN IX (Glossopharyngeal) | Greater cornu of the hyoid | Stylopharyngeus muscle |
| 4th & 6th Arches | CN X (Vagus nerve) | Thyroid and Cricoid laryngeal cartilages | Intrinsic muscles of the larynx, Cricothyroid |
General Histology: Epithelial Lining Patterns
Learn the precise cell tissue architecture found in different mucosal linings throughout the human body:
| Epithelium Type | Primary Locations | Core Functional Role |
| Simple Columnar | Stomach, Small Intestine, Large Intestine | Active secretion and absorption |
| Pseudostratified Ciliated Columnar | Trachea, Bronchi (Respiratory tract) | Clearance of mucus and foreign particles |
| Stratified Squamous Non-Keratinised | Esophagus, Cornea, Vagina, Oral cavity | Protection against mechanical abrasion |
| Transitional Epithelium (Urothelium) | Urinary Bladder, Ureters, Renal Pelvices | Allows distension and stretching without leakage |
FAQs Based on FMGE Strategy for Anatomy
Q1. Is it required to memorize origins and insertions of all the muscles in the FMGE?
Ans: Not at all. It would be a waste of time to learn everything about origins and insertions. All you have to do is concentrate on the nerve supply and the primary collective action of major compartments like the rotator cuff, muscles of the anterior compartment of the thigh, and muscles of mastication.
Q2. How to learn Neuroanatomy diagrams to match the new time-bound format?
Ans: You should concentrate on the identification of structures in the schematic figures, like the Circle of Willis, cross-section of the cavernous sinus, and brainstem sections. Practice using time-bound custom modules to develop your skill of recognizing a labelled structure and its associated clinical presentation in 45 seconds.
Q3. Can I skip Embryology and Histology to save time in the final weeks?
Ans: Do not skip them entirely. Despite seeming complex, the questions from it are extremely predictable, being asked again and again. Spend no more than 2 to 3 hours studying the Pharyngeal Arches, Neural Crest derivatives, and Types of Epithelium. In this way, it is easy for you to secure a few simple 3 to 4 marks.
Are you excited to test your anatomical recall capabilities visually? Open your Prepladder app and create a custom module, prepare 50 question IBQs for Upper Limb and Neuroanatomy only, and see what your score comes out to be!

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
1. Upper Limb: Plexuses & Clinical Nerve Lesions
Anatomy of the Brachial Plexus
Download the Academic PDF for FREE and Boost your Exam Prep
Upper Limb Nerve Deformities & Fracture Correlations
2. Lower Limb: Nerve Coordinates, Gates & Clinical Deformities
Lower Limb Peripheral Nerve Summary
3. Neuroanatomy: The Circle of Willis, Cranial Nerves & Dural Sinuses
Circle of Willis and Cerebrovascular Anomalies
Cranial Nerves & Cranial Foramina Lockouts
The Cavernous Sinus Anatomy
4. Head and Neck: Triangles, Glands and Key Spaces
5. Thorax: Coronary Circulation & Diaphragmatic Levels
Blood Supply of the Heart
The Diaphragm Openings & Associated Vertebral Levels
6. Abdomen: Hernias, Portocaval Anastomosis & Core Vessels
Inguinal Canal Anatomy & Hernia Differentiation
Portocaval Anastomosis & Portal Hypertension
7. Pelvis and Perineum: Spaces, Ligaments & Urinary Contours
8. Embryology & General Histology
Pharyngeal (Branchial) Arch Derivatives
General Histology: Epithelial Lining Patterns
FAQs Based on FMGE Strategy for Anatomy
Top searching words
The most popular search terms used by aspirants
- Anatomy Important Topics
- FMGE Anatomy Preparation