Cholinergic Drugs (Sympathetic & Parasympathetic system)
Feb 27, 2023

Autonomic Nervous System (ANS)
- It is the part of the nervous system which controls the involuntary functions.
- It consists of the different output from the central nervous system i.e. brain and spinal cord.
- ANS is divided into two parts, based on anatomy
| Sympathetic system | Parasympathetic system |
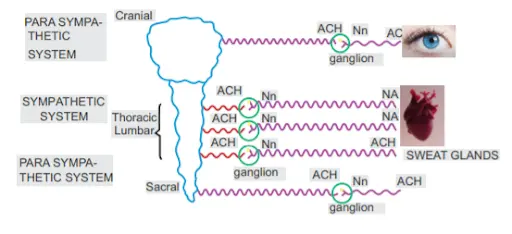
| Nerve fibres which originate from the thoraco-lumbar portion of spinal cord are called sympathetic nerve fibres. | Nerve fibres which originate from the Cervical or sacral portion of spinal cord are called parasympathetic nerve fibres. |
| Consists of Thoraco- lumbar outflow | Cranio – sacral outflow |
| Pre-ganglionic fibres are small and post-ganglionic fibres are long | Pre-ganglionic fibres are long and Post-ganglionic fibres are small |
| Ganglion is near the spinal cord | Ganglion is away from the spinal cord |
- All the pre-ganglionic fibres, whether they belong to the sympathetic system or parasympathetic system release the same neurotransmitter i.e. Acetylcholine.
- The receptor for this Ach is also the same i.e. NN receptor, present at the post ganglionic fibre.
- The post-ganglionic fibre carries the information to the organ.
- This fibre releases a neurotransmitter which acts on the receptors present in the organ
- The neurotransmitter is different for different fibres
- Parasympathetic system: Ach
- Since both pre-ganglionic and post-ganglionic fibres of parasympathetic system release Ach, it is also called Cholinergic system
- Sympathetic system: Nor-adrenaline
- The sympathetic system is also called Adrenergic system
- Exceptions
- Post ganglionic sympathetic fibres in sweat glands release Acetylcholine
- At renal blood vessels, the neurotransmitter secreted is Dopamine
- Parasympathetic system: Ach
Actions of Sympathetic & Parasympathetic system
|
Organ / Sympathetic system |
Parasympathetic system |
|
i. Heart : +++ (+ve chronotropic +ve dromotropic +ve ionotropic) |
-- (-ve chronotropic-ve dromotropic) |
|
|
|
ii. Bronchus: Broncho-dilation |
Broncho-constriction |
|
iii. GIT: Constipation |
Diarrhea |
|
iv. Bladder: ↓ Urine outflow |
↑ Urine outflow |
|
v. Glands: ↓ Secretions (but sweat ↑) |
↑ Secretions |
|
vi. Eye: Mydriasis (Dilation of pupil) |
Miosis (Contraction of pupil) |
|
vii. Sex: Ejaculation |
Erection |
- In the case of sexual system, both sympathetic and parasympathetic system complement each other
Previous Year Question
Question: Which of the the following action is expected on stimulation of muscarinic receptors? (AIIMS Jun 2020)
- Erection
- Ejaculation
- Increased contraction of cardiac muscles
- Bronchodilation
UNDERSTAND WITH EXAMPLE
- Point and Shoot: ‘Point’ means erection and ‘P’ for parasympathetic
- ‘Shoot’ means ejaculation and ‘S’ for sympathetic
Parasympathetic System
- It originates from cranio-sacral nerves
- Cranial Nerves
- III, VII, IX, X are parasympathetic
- Rest all are autonomic nerves
- No cranial nerve is sympathetic
- Sacral Nerves : 2,3,4 are parasympathetic
- Also called cholinergic system because both the pre-ganglionic and post-ganglionic fibres secrete Ach.
- Acetylcholine synthesis
- First step is uptake of choline from outside the neuron
- This choline forms Acetylcholine inside the neuron. This Ach is stored inside the vesicle where it remains safe
- When the impulse arrives, this Ach is released into the synapse and starts stimulating the post-synaptic receptor.
- To stop the action of Ach after stimulation of receptors is complete, the Ach is broken down by enzyme Acetyl cholinesterase
- Rate limiting step: Uptake of choline
- Regulation of Ach level in the synapse
- Inhibit choline uptake
- Hemicholinium: It inhibits the uptake of choline in the neuron so parasympathetic action decreases
- Inhibit uptake of Acetylocholine
- Vesamicol: It inhibits the uptake of Acetylcholine in the vesicles
- Inhibit release of Acetylcholine
- Botulinum toxin: It inhibits the release of Acetylcholine from the neuron into the synapse
- Inhibit Ach breakdown
- Physostigmine: It increases the level of Ach by inhibiting its breakdown via Acetylcholine esterase (AchE)
- Inhibit choline uptake
- The 1st three drugs have actions opposite to the parasympathetic system
- The last drug physostigmine has similar action as the parasympathetic system
Cholinergic Receptors
- The cholinergic receptor are of two types :
|
Muscarinic (M) |
Nicotinic (N) |
|
|
Drugs acting on these receptors
- Parasympathomimetic drugs
- Their action is similar to the parasympathetic nervous system
- Parasympatholytic drugs
- These drugs block the action of parasympathetic system

PARASYMPATHOMIMETIC DRUGS (aka Cholinergic Drugs)
- These drugs mimic the actions of parasympathetic system
- They are also called cholinergic drugs
- These are of two types
- Directly acting: These are the drugs that directly stimulate the Nicotinic and Muscarinic receptors
- Indirectly acting (AchE inhibitors): These drugs inhibit AchE, so Ach cannot be broken down and its level increases
- Directly Acting drugs
- Ach
- Carbachol
- Bethanechol
- Methacholine
- Pilocarpine
- AchE present in synapse: True AchE
- AchE present in plasma: Pseudo AchE or Butryl ChE
- If we give Ach clinically, as soon as it reaches the blood, it is broken down by the Pseudo ChE. Thus Ach is very short acting and not suitable to be used clinically
- Bethanechol mainly works on the urinary bladder (M3). It is used in treatment of Atonic bladder
- Methacholine acts on the myocardium (M2). It is used in Tachyarrhythmia
- Pilocarpine acts on the pupil (M3). It is used for treatment of glaucoma
- These drugs act on muscarinic receptors. None of these 3 drugs acts on Nicotinic receptors
- Carbachol is the only drug in the category which acts on both muscarinic as well as Nicotinic receptors
- Cevimeline is a recent directly acting cholinergic drug that acts on M3 receptors. It stimulates the glands and increases secretions, so used in treatment of Sjogren’s syndrome
- Indirectly acting Cholinergic drugs (AchE inhibitors)
- These drugs are inhibitors of AchE. They may be of 2 types
|
Reversible AchE # |
Irreversible AchE # |
|
|
Reversible AchE#
- These are of 2 types
- Lipid soluble: Physostigmine
- Water soluble: Neostigmine
1. Lipid soluble drugs
- Lipid soluble drugs will cross the membranes and water soluble drugs cannot cross the membranes
- So physostigmine can be used in GIT, Eye or CNS conditions and Neostigmine cannot be given as it won’t get absorbed
- Physostigmine is lipid soluble because it is a tertiary amine and tertiary amines are lipid soluble
- Also, Neostigmine is water soluble because it is a quaternary amine and quaternary amines are water soluble
- Physostigmine is used for treatment of glaucoma. It leads to miosis in the eye.
- Physostigmine can cross the blood brain barrier, so can be used for treatment of Atropine poisoning. Atropine is a muscarinic blocker, so in atropine poisoning muscarinic receptors are not working
- Atropine blocks the receptors both inside the brain and outside the brain because it is lipid soluble. Therefore, Physostigmine is DOC for Atropine poisoning
Basal Nucleus of Meynert
- Basal nucleus of Meynert is the area in the brain that contains plenty of Ach and is a major area of cholinergic supply.
- This area is involved in memory - it is responsible for acquiring and retaining the memory
- So Ach is required for memory
- If there is death of neurons in the Basal area of Meynert, there is loss of memory, i.e. Dementia. This death of neurons occurs more in old age people, so this is called Senile Dementia or Alzheimer’s dementia. It commonly occurs after 60 yrs of age
- If we give Physostigmine for Alzheimer’s disease, it affects the muscarinic receptors outside the brain too. So it will improve the memory but also lead to various side effects
- Tacrine is also a lipid soluble AchE# like Physostigmine. But unlike Physostigmine, Tacrine has >99% entry in the brain, so it will improve memory without causing significant side effects
- But problems with Tacrine are – it is short acting and hepatotoxic. Also it needs to be given 4 times a day and Alzheimer’s patients cannot remember to take the drug 4 times a day, so Tacrine is not DOC anymore.
- New drugs for Alzheimer’s
- Lipid soluble AchE# with >99% entry in brain, similar to Tacrine
- Donepezil
- Rivastigmine
- Galantamine
- Lipid soluble AchE# with >99% entry in brain, similar to Tacrine
- But unlike Tacrine, these drugs are long-acting and do not cause liver damage, so these have become the DOC for Alzheimer’s disease
- Other drugs used for Alzheimer’s disease
- NMDA#
- Memantine: Blocks the receptors of Glutamate so it improves memory and can be used for Alzheimer’s disease
- Aducanumab: It is a monoclonal antibody against Aβ2 amyloid, which is causing destruction of neurons. So it treats the underlying cause of Alzheimer’s disease
- NMDA#
Water soluble drugs
- Water soluble AchE# drugs are
- Neostigmine
- Pyridostigmine
- Edrophonium
- These are preferred when we want action outside the brain. These are water soluble so won’t cross the blood brain barrier
- Uses
- Myasthenia gravis
- There is formation of antibodies against NM receptors, so less stimulation of NM receptors occurs. This leads to muscle weakness
- Most commonly involved muscle is Levator Palpabrae Superioris (LPS), leading to Ptosis
- NM receptors require optimal stimulation to work normally. If there is over – stimulation of these receptors it leads to cholinergic crisis
- This is opposite to myasthenia gravis. The treatment is also opposite in both the conditions
- To differentiate between the 2 conditions, we give Edrophonium I.V. It inhibits AchE and leads to ↑ level of Ach. This Ach stimulates the NM receptors. As a result, if the condition improves, the diagnosis is myasthenia gravis. But if the condition worsens, it is diagnosed as Cholinergic crisis
- Edrophonium is used because it is very short acting. So if the condition worsens, it will not last beyond 10min. So it is DOC for diagnosis of Myasthenia gravis. This test is known as Edrophonium test or Tensilon test
- For treatment of Myasthenia gravis, we need long acting drugs like Neostigmine and Pyridostigmine
- Pyridostigmine is slightly longer acting than Neostigmine
- Apart from inhibiting AchE, these drugs also directly stimulate the NM receptors.
- Neostigmine is given along with Atropine for the treatment of Myasthenia gravis. Atropine blocks the muscarinic side effect caused by neostigmine
- Cobra bite
- Cobra is a neurotoxic snake. Its venom goes to the NMJ and binds to the NM receptors. This leads to muscle weakness
- The treatment of choice for any snake bite is Anti-Venom. But it is not available in every hospital, so we can treat the patient symptomatically by giving Neostigmine + Atropine
- Reversal of muscle relaxants
- Drugs which block the NM receptors like Atracurium, Pancuronium lead to muscle relaxation. These belong to the category of Non-Depolarizing Muscle Relaxants (NDMR)
- These drugs are used for surgery. Their action is long lasting, so we need to give a drug to reverse their action after the surgery is over
- We use Neostigmine + Atropine for reversal of muscle relaxants. Atropine is added to prevent the muscarinic side effects
- Postoperative paralytic ileus
- It is a muscarinic use of neostigmine
- After any abdominal surgery, we keep the patient NPO (Nil per oral) because the ileum is not working. We come to know that the ileum is working again, after passage of flatus
- In some people, flatus is not passed and the ileum does not start working again. This condition is called Paralytic ileus
- So we need to stimulate the ileus from outside. We give Ach to stimulate the M3 receptors on the ileum. This is done by giving neostigmine which increases the level of Ach.
- We don’t add Atropine with neostigmine in this case because Atropine will block the M3 receptors
- Bethanechol can also be used
- Post-op. urinary retention
- This is similar to post-operative paralytic ileus, so we give Neostigmine to stimulate the muscarinic receptors on the bladder
- Atropine is not used here
- Bethanechol can also be used for this condition
- Myasthenia gravis
Irreversible AchE#
- Ecothiophate is an example
- It can be used as eye drops for miosis
- These drugs can be divided into 2 types
|
Organophosphates |
Carbonates |
|
|
- Endrin is an organo-chlorine, not an organo-phosphate
- These drugs are not used clinically
- They are used commercially as insecticides, pesticides, etc. by farmers
- So they can cause poisoning in farmers because they are highly lipid soluble
- They permanently block the AchE and thus increase Ach. This leads to various muscarinic effects like:
- M1 : ↑HCl
- M2 : ↓HR, ↓BP
- M3 : Pinpoint pupils
Increased secretions
Severe diarrhea
Urinary incontinence
Broncho-constriction
- To treat these poisonings we give Atropine. It is the DOC because it blocks the muscarinic receptors.
- Atropine is given by I.V. route because it is an emergency. The dose is repeated every 5 min because the amount of poison in the body is not known. So we repeat the dose till we see some signs. These signs are called Signs of Atropinization
- Signs of Atropinization are
- Mydriasis : When the pupil dilates and we see reversal of atropinization
- Decrease in secretions
- HR >100 :Tachycardia occurs.
- MC sign is Mydriasis
- Most reliable / specific sign is Decreased Secretions
- Atropine can reverse all the symptoms of OP poisoning except muscle weakness. In most cases, muscle weakness is seen after other symptoms have subsided.
- Other drugs given for poisoning are : AchE Reactivators (aka Oximes)
AchE Reactivators (Oximes)
- Pralidoxime (PAM)
- Diacetyl monoxime (DAM)
AchE has 2 sites
- Esteratic site
- Anionic site
- Ach binds to the Esteratic site and it is broken down very fast. The breakdown is so fast that this site is considered always free
- When Organophosphates bind to the esteratic site, they do not break down and do not leave, so when Ach comes it cannot bind and thus not broken down. So Ach level increases.
- We need to remove the OP from this site so that AchE is available again
- We give Oximes which bind to the Anionic site. Then they form a bond with the OP on the esteratic site. This bond is very strong and breaks the bond between the OP and the esteratic site. So the esteratic site is now free.
- In the case of Carbamates
- Carbamates are big molecules and occupy both esteratic and anionic sites
- So, oximes cannot bind to the anionic site and thus cannot reverse the poisoning caused by carbamates
- Oximes are C/I in carbamate poisoning
- Pralidoxime has peripheral action only whereas Diacetyl monoxime has dual action- brain as well as periphery
- If oximes are given early on in the poisoning, they work efficiently. But if we give them very late, they cannot work properly because the bond between OP and the esteratic site has become too strong to break. This is called the Ageing of Enzymes.
If you have any doubts or questions on this topic, download the PrepLadder app and learn more about this important anesthesia topic from in-depth video lectures and NEET PG study material.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Autonomic Nervous System (ANS)
Actions of Sympathetic & Parasympathetic system
Parasympathetic System
Drugs acting on these receptors
PARASYMPATHOMIMETIC DRUGS (aka Cholinergic Drugs)
Reversible AchE#
Basal Nucleus of Meynert
Water soluble drugs
Irreversible AchE#
AchE Reactivators (Oximes)
AchE has 2 sites
Top searching words
The most popular search terms used by aspirants
- NEET PG Anesthesia