Systemic Lupus Erythematosus
May 30, 2023

A chronic autoimmune illness known as lupus, sometimes known as systemic lupus erythematosus (SLE) or simply "lupus," can result in pain and swelling all over your body.
Your immune system battles against itself when you have an autoimmune disease. The immune system is meant to protect the body from potential threats, such as infections, but in this instance, it attacks healthy tissue.
Read this blog further to get a quick overview of this important topic for dermatology and ace your NEET PG exam preparation.
RISK FACTORS For SLE:
Some risk factors are mentioned below which can lead to SLE:
- Genetic factors - HLA DQ polymorphism and Deficiency of complement proteins (C1 /C2 /C4)
- Environmental factors- UV rays, Female predominant (hormonal and genes specifically located in 'X' chromosome)
- Drugs-Immunologic factors like Hyper activation of B & T-Lymphocyte
Most Common Presentation of SLE:
- Musculoskeletal manifestation is pain
- Hematological presentation is anemia
- Subsequently skin manifestations like Malar rash can also be found.Malar flush is a presentation with mitral stenosis so it should not be confused for malar rash.
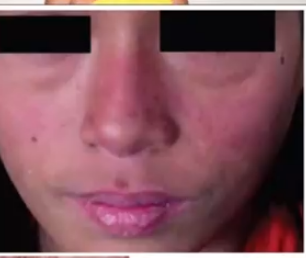
- Butterfly rash- Erythematous rash can be found on the cheek involving bridge of nose but in this the Nasolabial folds are spared . All rashes in SLE show photosensitivity, the burning sensation persists even after sun exposure and coming under shade. Malar rash as it is seen on malar eminence. Erythematous rash is with raised margin. It is Also seen on Hands and V of neck, do not confuse this with seborrheic dermatitis, In seborrheic dermatitis yellow greasy flakes that peel off are seen and they begin from nasolabial folds.
- Other dermatological manifestations

Subacute cutaneous lupus erythematosus have Psoriasis like lesions. Discoid lupus have circular lesions and peripheral erythematous lesions and show Center scarring which is known as atrophic scarring. In this the Dermal appendages are lost and it may be confused for Fungal infection. But fungal infections show central clearing. Atrophic scarring seen in discoid lupus but non-scarring alopecia is associated with SLE .
ACR 2019 is the diagnostic criteria that has higher sensitivity and is specificity used for SLE.
Autoantibodies involved in SLE:
1. ANA- It has 98 % sensitivity therefore it is most sensitive. It is not only positive in SLE but we can find ANA in scleroderma and sjogren's syndrome as well.
2. Anti smith antibody- it is the Most specific antibody found in SLE.
3. Anti ds DNA - As SLE is an autoimmune condition it shows waxing and waning course. The value of anti ds DNA tends to correlate with disease activity. Anti ds DNA value can be used to check if SLE worsens / gets better during pregnancy and to see response when treated with steroids.
4. Anti Ro antibody - anti-SS-A antibody - this antibody is responsible for photosensitivity. Acute, chronic, psoriatiform or discoid - all rash in SLE shows photosensitivity . All lesions worsen with sunlight. anti Ro can spread Transplacentally and can Causes Damage to AV node in fetus This causes SA node to control atria and Bundle of his to control ventricle
Leads to Complete heart block and the Fetus develops neonatal lupus leading to Severe bradycardia at birth. A Bundle of his can fire 15 - 30 / minute only . Child develops Syncope and May be Unresponsive showing Sluggish MORO reflex.
5. Anti Lupus anticoagulant - anti SS- B antibody. It Decreases risk of nephritis.
6. Anti Histone antibody - This antibody is found in drug induced lupus. It will not develop lupus nephritis or lupus cerebritis so its Prognosis is better. Once a drug is discontinued then after 8 weeks they resolve on its own. Drugs used are:
- Sulfa drug
- Hydralazine
- Isoniazid
- Procainamide - it is a Antiarrhythmic agent and is Used in Wolff parkinson white , Lown-Ganong-Levine syndrome
7. APLA - antiphospholipid antibody syndrome
- Anti cardiolipin antibody
- Anti b2 glycoprotein antibody
- Lupus anticoagulant
8. Autoerythrocyte antibody- The Common anemia in SLE is anemia of chronic disease. But autoimmune hemolytic anemia can also occur.
9. Antiplatelet antibody- associated with Thrombocytopenia and shows Petechiae around ankles.
10. Anti neuronal antibody- it Cross Blood brain barrier and Cause Cerebral edema.
11. Anti glutamate receptor antibody
12. Anti ribosomal P antibody- it causes Cause psychosis
Clinical Features of SLE
- Malar Rash Sparing Nasolabial Fold.
- Discoid lupus erythematosus- in this the Periphery is hyperpigmented, erythematous whereas the Center shows atrophic scarring and in this the dermal appendages are lost. In this we can find Non scarring alopecia and Discoid central scarring.

- Serositis - It Affects lung and heart
| Lung | Cardiac |
| Pleuritis → pleural effusion | Pericarditis → effusionEcho- bag of water appearance in pericardial effusion |
| Shrinking lung syndrome Timed vital capacity ↑ | Libman sacks endocarditis |
| Pleuritic chest pain - worsens with inspiration | ECGST elevationConcave upwards |
- Libman sacks endocarditis
It is a condition in which Sterile vegetations of fibrin deposits occur predominantly on inferior surface involvement. Inferior to valves are chordae tendineae. In Libman-Sacks there is malfunction of chordae tendineae which leads to hampering of valve integrity. This leads to mitral regurgitation
- Oral aphthous ulcers
It is Also seen in stress , or due to constipation and can be Idiopathic as well. These ulcers Usually resolve with Topical benzocaine jelly. In SLE aphthous ulcers are Recurrent.
There may be crops of aphthous ulcers,some develop and resolve and then come again on the same side or opposite side.They are usually painless. Recurrent aphthous ulcer and recurrent vulvar ulcers are painful and are presentation of Behcet’s disease
- Alopecia - non scarring
- Synovitis
It causes Joint pain and it is the most common presentation of disease. It is associated with low grade fever. In this 2 or more than 2 joints are affected. These joints could be small or large , symmetrical or asymmetrical. Soft tissue swelling may also be present. Patients could complain of knee joint pain one day and the next day complain of elbow or wrist joint pain. Non-erosive arthritis is also seen in rheumatic fever. Deformities can also occur but are rare.
- CNS involvement
The most common CNS manifestation is cognitive defects. It can also lead to Lupus cerebritis. Antineuronal antibodies cause cerebral edema, headache and seizures.Dexamethasone reduces cerebral edema. Psychotic features are associated with anti Ribosomal P antibodies.
- Renal involvement
It can lead to Lupus nephritis which contributes to mortality. In this we can also find hematuria which is a cola colored urine. It can also lead to hypertension, End Stage Renal Disease, Uremia , hyperkalemia and metabolic acidosis. On Urine microscopy we can find hematuria that is RBC > 5/ hpf and dysmorphic RBC due to glomerular damage. RBC in normal urine is 3-5/hpf. Freshly passed urine when centrifuged shows sediment containing RBCs, C3 is low, increased Creatinine and increased blood urea nitrate.
- Anemia
Commonly in SLE we can find anemia or chronic disease. We can also find normocytic normochromic anemia. Other causes of anemia are autoimmune hemolytic anemia. In this the Antibodies are formed against erythropoietin and also against the receptor in case of Impaired response of erythropoietin so the antibody acts against the receptor. Antibodies destroy RBCs.
- Immunological
- Antibodies
- Anti Smith antibody - most specific
- Anti ds DNA =course and progression of disease
- Low C3 and C4
- antinuclear antibody
.jpg)
Criteria For Diagnosis of SLE:
- Discoid lupus erythematosus
- Serositis - pleuritis and pericarditis
- Oral aphthous ulcers - painless
- Non scarring alopecia
- Sinovitis- 2 or more than 2 joints involved or intermittent polyarthritis
- Brain - cognition defects, psychotic
- Renal - Lupus Nephritis or ESRD
- Anemia - anemia of chronic disease , autoimmune hemolytic anemia. Autoantibody damage self WBCs leading to leukopenia and if And platelets are damaged it leads to thrombocytopenia
- Immunological
- Direct coombs test
- Positive in AIHA
- Anti smith antibody
- ANA
- Lupus anticoagulant
- ELISA Anticardiolipin - ACL - give false positive VDRL
- Anti B2 Glycoprotein
- Low C3 and C4
For diagnosis
Out of the above a total of 4 + features should be present or at least 1 clinical and 1 immunological feature should be present or one clinical + 3 immunological features should be present.
Latest ACR criteria - 2019
It Includes Fever. These criteria are almost the same as the previous one. In this the Highest weightage is given to biopsy that is 10 points. Taking the highest rating from each if more than 1 are present under one category like hematological or neurological or cutaneous. For Diagnosis of SLE a total score must be more than 10 along with presence of ANA. The drug of choice for SLE in pregnancy is hydroxychloroquine. In this the Steroids are not given because Steroids are deactivated by placental enzymes. So, hydroxychloroquine is given in photosensitivity and pregnancy.
To scale up your NEET PG preparation with the best-in-class video lectures, QBank, Mock Tests and more, download the PrepLadder App!
Download PrepLadder's NEET PG preparation app for Android
Download PrepLadder's NEET PG preparation app for iOS

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
RISK FACTORS For SLE:
Most Common Presentation of SLE:
Autoantibodies involved in SLE:
Clinical Features of SLE
Criteria For Diagnosis of SLE:
For diagnosis
Latest ACR criteria - 2019
Top searching words
The most popular search terms used by aspirants
- NEET PG Dermatology
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial