Juvenile Nasopharyngeal Angiofibroma: Site of Origin, Staging
Jul 21, 2023

Juvenile nasopharyngeal angiofibroma is exclusively seen in the juvenile age group. Angiofibroma is a tumor filled with lots of blood vessels and fibrous tissue. It is a benign and a rare tumor but also the most common tumor of the Nasopharynx. It is exclusively seen in males because it depends upon testosterone.
.jpg)
Site of Origin Of Juvenile Nasopharyngeal Angiofibroma
The most common site of origin is from the sphenopalatine foramen (near the posterior wall of the maxillary sinus). Sphenopalatine foramen is located 8-10 mm behind the posterior end of the middle turbinate. Another site of origin are:
- The anterior wall of the sphenoid sinus
- Roof of nasopharynx
- Lateral wall of the nasopharynx
Staging Of Juvenile Nasopharyngeal Angiofibroma
Stage Description IA Limited to nose and nasopharyngeal area IB Extension into 1 or more sinuses IIA Minimal extension into pterygopalatine fossa IIB Occupation of the pterygopalatine fossa with or without orbital erosion IIC Infratemporal fossa extension with or without cheek or pterygoid plate involvement IIIA Erosion of the skull base (middle cranial fossa or pterygoids) IIIB Erosion of skull base with intracranial extension with or without cavernous sinusinvolvement
Clinical Feature of Juvenile Nasopharyngeal Angiofibroma
Below are mentioned some of the clinical features of juvenile nasopharyngeal angiofibroma
- Bleeding- Recurrent unprovoked profuse epistaxis.
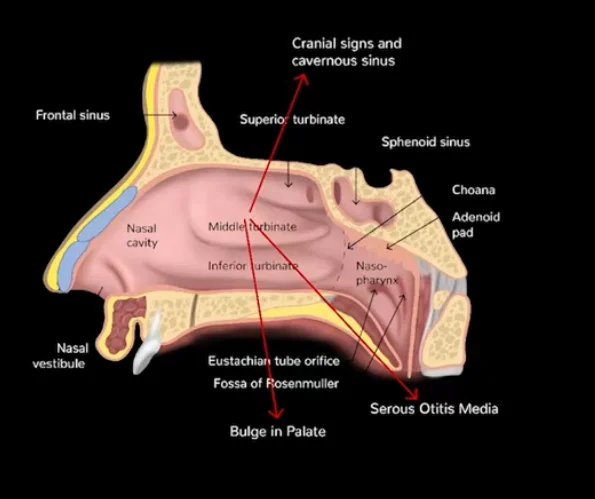
- Nasal obstruction and Eustachian tube obstruction
- Unilateral serous otitis media and conductive hearing loss (Eustachian tube obstruction)
- Frog face deformity

- Hyponasal speech
- Cranial spread- Cranial involvement (2nd,3rd,4 th,5 th,6th CN palsy). Extension into sphenoid and cavernous sinus causing nerve palsies
Clinical Examination Of Juvenile Nasopharyngeal Angiofibroma

- Anterior rhinoscopy shows Globular pink mass in the posterior part of the nasal cavity, septum being pushed to the opposite side.
- Posterior nasal examination shows Pink to purple globular mask with dilated blood vessels.
- Probe test and Digital palpation of tumor is contraindicated.

Diagnosis Of Juvenile Nasopharyngeal Angiofibroma
Diagnosis can be made with the help of following methods:
- History
- Examination:
- X-ray neck lateral view
- X-ray PNS
- CECT scan – IOC
- MRI
- Angiography
- No biopsy
- Plain X-ray/CT scan: Anterior bowing of posterior wall of the maxillary sinus which is known as Holmann Miller sign.

- Hondusa’s sign: increase in distance between maxillary sinus and mandible on CT scan.
- Opacification of sphenoid sinus.
Role of CT scan
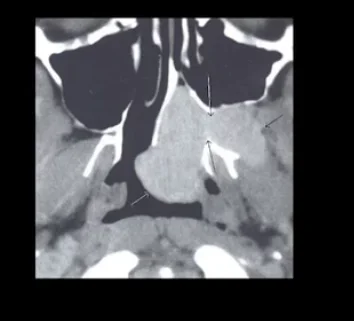
CT diagnosis is based on two constant features
- Mass in the nose and pterygopalatine fossa.
- Erosion of bone behind the sphenopalatine foramen at the root of the pterygoid plate.
When the wedge of the pterygoid is eroded so the medial and lateral pterygoid plate look like a separate plate, that is called the Chopstick sign.
Role of MRI
- MRI accesses the relation of the tumor to the critical structures such as the internal carotid artery, cavernous sinus, and pituitary gland.
- Recurrent and residual tumors are the best appreciated on the MRI.
Role of Angiography
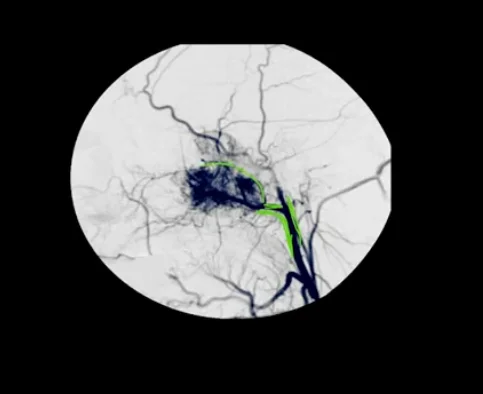
Angiography provides information on the specific blood supply of the tumor. The most common blood vessel supplying the tumor is internal maxillary artery. It is also used as treatment with embolization.
What Is The Blood Supply Of Juvenile Nasopharyngeal Angiofibroma?
The internal maxillary artery is the most common vascular source from which juvenile nasopharyngeal angiofibroma arises. Other known vessels include ascending pharyngeal artery
When is the biopsy done for Juvenile Nasopharyngeal Angiofibroma?
No biopsy is done for juvenile nasopharyngeal angiofibroma. Only when radiotherapy is contemplated due to the inoperability of the tumor is one exception when the biopsy is done.
Treatment Of Juvenile Nasopharyngeal Fibroma
Treatment of choice for juvenile nasopharyngeal angiofibroma is surgery with preoperative embolization. To decrease vascularity
- Embolization is done 24 to 48 hours before surgery
- A course of estrogen therapy (stilbesterol 2.5 mg thrice daily for three weeks)
- Cryotherapy
Role of Radiotherapy
Radiotherapy is used when there is
- Intracranial involvement
- Direct blood supply from internal carotid artery
- Unresectable tumor
- Multiple recurrences may be good candidate for radiation therapy
Recurrence rate of 20-30% can expected with radiation therapy alone. Newer techniques in radiotherapy treatment such as intense modulated conformal radiotherapy (IMRT) and gamma knife have shown good results.
Hormonal Therapy & Chemotherapy
Diethylstilbestrol with flutamide is used because it is testosterone dependence. Chemotherapy for residual/recurrent disease includes doxorubicin, vincristine, and dacarbazine.
Download the PrepLadder App and get the best neet pg online coaching with world-class video lectures, QBank, Mock Tests and more!
Download PrepLadder's best app for neet pg preparation for Android
Download PrepLadder's best app for neet pg preparation for ios

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Site of Origin Of Juvenile Nasopharyngeal Angiofibroma
Staging Of Juvenile Nasopharyngeal Angiofibroma
Clinical Feature of Juvenile Nasopharyngeal Angiofibroma
Clinical Examination Of Juvenile Nasopharyngeal Angiofibroma
Diagnosis Of Juvenile Nasopharyngeal Angiofibroma
Role of CT scan
Role of MRI
Role of Angiography
What Is The Blood Supply Of Juvenile Nasopharyngeal Angiofibroma?
When is the biopsy done for Juvenile Nasopharyngeal Angiofibroma?
Treatment Of Juvenile Nasopharyngeal Fibroma
Role of Radiotherapy
Hormonal Therapy & Chemotherapy
Top searching words
The most popular search terms used by aspirants
- NEET PG ENT
- NEET PG ENT Preparation