Rapid ECG Review: High-Yield Cardiology Tracings for NEET PG Medicine
Aug 29, 2025


ECG Interpretation (Myocardial Infarction)
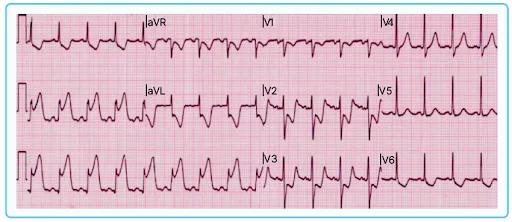
- ECG image with ST elevation in LEAD II, III, and aVF and reciprocal changes of ST depression in V1,2,3,4 indicating Inferior wall MI.
- In lead II:
- P wave present, no Q wave
- Characteristic ST elevation present - Tomb Stone Pattern (ST elevation is convex in an upward direction)
- In Inferior wall MI, the thrombus mainly presents in RCA
ECG Findings in MI (Myocardial Infarction)
Hyperacute T wave (Earliest ECG finding)
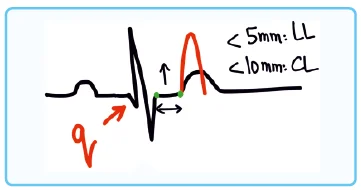
- Normal size criteria of T wave:
- Vertical height is <5mm in limb leads & <10 mm in chest leads
- More than normal size of T wave - Hyperacute T wave
- Indicates Myocardial Ischemia.
- Develops within seconds of infarction
2. ST elevation
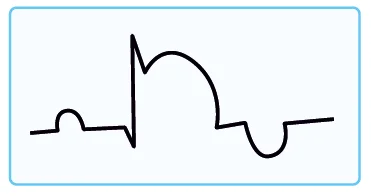
- Significant ST elevation:
- For Male patients: The rise is ≥ 2mm
- For female patients: The rise is ≥1.5mm
- Also called current of injury.
- Indicates Myocardial injury.
- Myocardial injury is best identified by cardiac biomarkers
- Develops within minutes of infarction
3. Q waves/ Pathological Q waves
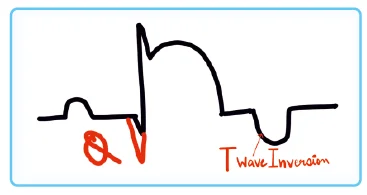
- In a normal individual, the Q wave is within one small square
- Indicates Cell Death or Previous MI
- A deep Q wave persists for the whole life.
- Usually develops after >1hr of infarction
4. T wave Inversion
ST elevation is associated with a T wave inversion.
Tombstone Pattern/ Pardee sign ECG
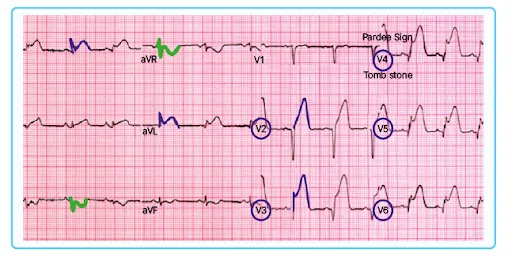
- Tombstone pattern/ Pardee sign (Pardee waves refers to the symmetric inversion of T waves during an acute coronary syndrome or myocardial ischemia.)
- Significant ST elevation present in V2, V3, V4, V5,V6, Lead I, aVL and reciprocal change ST elevation is present in Lead III, aVR
- The above findings indicate: Extensive anterior wall MI
- High risk of developing Cardiogenic shock, Pulmonary edema, and Sudden cardiac death
- Sudden cardiac death: Death within 1 hour of being seen or heard. It could be Ventricular fibrillation or Pulseless Ventricular Tachycardia (PVT) and need defibrillation.
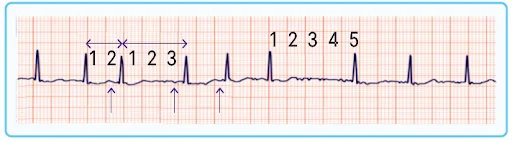
Sinus Arrhythmia ECG

Normal sinus rhythm with variable R-R interval that is not tachyarrhythmia is known as Sinus arrhythmia. Occurs as a result of vagal tone variation which is produced by the phases of respiration.
- ECG shows variable RR intervals like in the above figure.
- Here HR is varies from 100 to 75bpm (this is not tachyarrhythmia: HR>100bpm)
- P wave with QRS complex present - normal sinus rhythm.
- Normal sinus rhythm + Varying HR = Sinus arrhythmia.

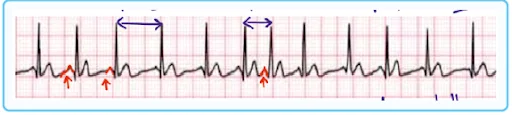
Atrial Fibrillation ECG

- An ECG showing both increasing and decreasing variations of HR with an absence of a P wave and the presence of twitching indicates Atrial Fibrillation.
- Due to atrial twitching, clots develop in the Left Atrial
- Appendage is seen.
- Blockage in the brain causes stroke
- Blockage in the mesenteric arteries causes infarction of bowel with lower GI bleeding presenting as very severe abdominal pain, and if not identified will lead to gangrene of the intestine
- There is a variable R-R interval
- The pulse in AF is often described as irregularly irregular.
- Atrial Fibrillation is the most common sustained arrhythmia
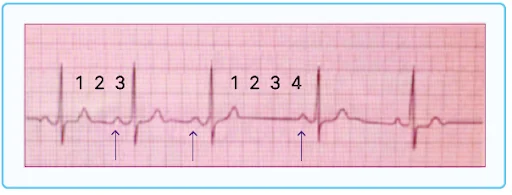
Multi-Focal Atrial Tachycardia ECG
- Patient with COPD with recurrent episodes of palpitations and dizzy spells.
- P waves are present - variable morphology/height
- ≥ 3 different varieties of P wave should be present
- Variable R-R interval (HR >100/min)
- Rx: DOC: Verapamil
- DC Shock is Contraindicated.
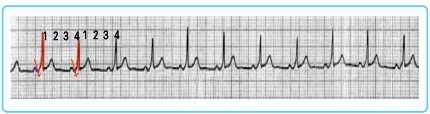
Atrial Flutter ECG
- Atrial flutter is a variant of Atrial fibrillation, only the site of heart involvement is different.
- Characteristic ECG finding: Saw Tooth Pattern.
- The macro re-entrant circuit around the cavotricuspid isthmus in the right side of the heart is responsible.
- Rx:
- Rate control with esmolol
- Anticoagulants
- Ibutilide
- If Ibutilide fails - Low-intensity DC shock with 25-50 J.
Paroxysmal Supraventricular Tachycardia ECG
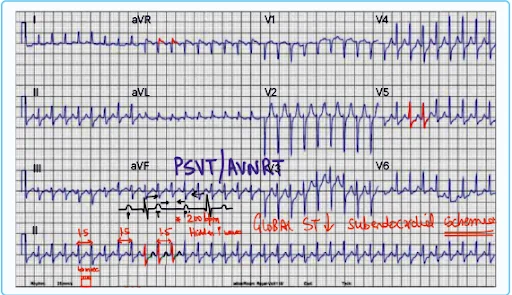
- Based on the HR in lead 2, the ECG shows tachyarrhythmia.
- Constant R-R interval
- QRS is on the lower side of the normal
- Global ST depression is present - Evidence of sub-endocardial ischemia.
- Merged P and T wave - Hidden P wave
- Also known as AV nodal re-entrant tachycardia (AVNRT) i.e., the narrow QRS complex tachycardia
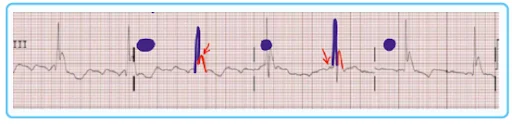
Wolf Parkinson White (WPW) Syndrome
ECG findings:
- There is change in the slope of the upswing of R wave - Delta waves.
- Short PR interval because of fast conduction in the heart (PR interval is inversely related to HR)
- ‘q' wave is absent - Since the current is not involving the AV nodal pathway and bundle of HIS
- Change in the upswing of R wave - Delta waves
- Broader RS complex:
- Delta wave contributes to a broader RS complex
- Intermyocyte conduction: The current travels through the myocytes (slower) instead of the Purkinje fibers (Fastest conducting fiber in the heart)
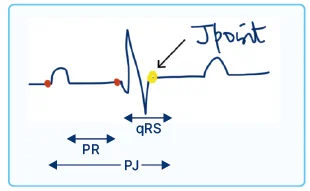
- PJ interval remains normal
- PJ= (↓) PR+ (↑) qRS
- The amount of PR reduction is equal to the increase in the RS complex
Hypothermia ECG findings
- Prolonged PR interval - due to slowing of the heart in hypothermia.
- An inverted P wave might be present - due to AV node firing the atria retrogradely
- A deflection/notch in the downswing of R wave - Osborn wave
- Ideal site for checking core temperature: Pulmonary Artery (invasive)
- Preferred site for checking core temperature: Lower esophagus
Ventricular Tachycardia ECG findings
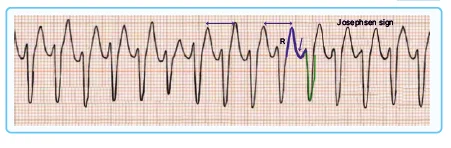
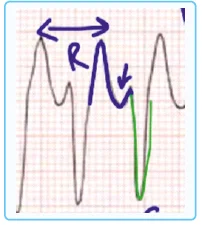
- HR ≃ 200 bpm
- Shortened R-R interval
- Broad qRS complex (Normal qRS complex is 2-2.5 small squares i.e., 80 to 100 milliseconds)
- Tachycardia with Broad qRS complex indicates VT
- All of the broad qRS complexes are monomorphic. Therefore, the given ECG shows Monomorphic VT
- Josephson Sign: A slight notch which is exclusively noted in VT
Hyperkalaemia ECG Findings
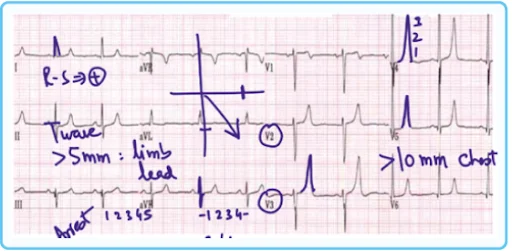
- HR >60 bpm.
- Tall-tented T waves are present (>10mm in chest leads, >5mm in limb leads).
- In hyperkalemia, ECG is not reliable. It is just supportive evidence.
- Serum electrolytes - more reliable
- Increased R-R interval - K+ slows the heart
- ST elevation is seen
- The amplitude of the P wave decreases and gradually disappears.
- PR interval increases and the broad QRS complex merges with T wave - the Sine wave pattern. Occurs just before diastolic arrest
- Hyperkalemia can lead to death by causing diastolic arrest (K+ slows the heart)
Bradyarrhythmias ECG Findings
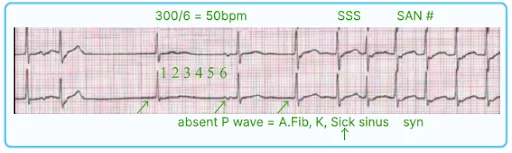
- No. of squares between R-R interval increases
- P wave is not deciphered or it is inverted which indicates malfunctioning of the SA node
- Heart rate = 300/60 = 50bpm
- SA node is not functioning properly (SA node normally fire - 60-100 bpm)
- On exertion - heart will not be able to generate the required amount of cardiac output leading to a syncopal episode
Second-degree Heart Block

Mobitz I or Wenckebach phenomenon
- Increasing trend of the PR interval (starting from P to the starting of the Q wave, it is not till the R wave)
- There is a P wave but no qRS complex
- There is missed beat experienced by a person who feels their own pulse
- Subsequently, there is a reset in heart rhythm and a serial prolongation of the PR interval followed by a missed beat.
- There is slow conduction via the AV node
Mobitz II heart block
- The PR interval for 1st , 2nd and 3rd time is constant
- Then there is a P wave followed by a missed beat, then again rhythm is reset
- The PR interval that comes subsequently will be almost of the same size
Third-degree heart block/Stokes-Adam syndrome
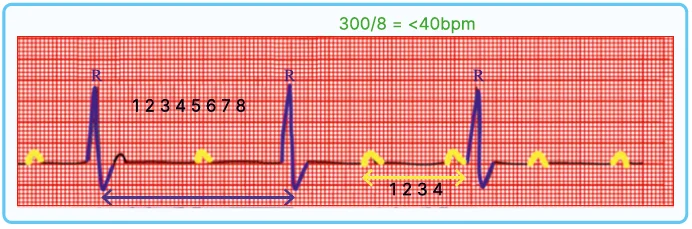
- R-R interval here is increased
- Heart rate ˂ 40 bpm
- QRS complex is relatively broad
- There is an A:V dissociation: No. of R waves and P waves do not match
- People with Stokes Adam syndrome will have hampering with the quality of their life
- Dual chamber/dual lead pacemaker is used on a priority
- Patients could have 'a' wave in JVP or frog waves in the JVP
- There is no conduction via AV node
Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Smarter Video Lectures also in हिंglish, Game Changing Qbank, Audio QBank, Structured Notes, Treasures, Mock test for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
ECG Interpretation (Myocardial Infarction)
ECG Findings in MI (Myocardial Infarction)
Hyperacute T wave (Earliest ECG finding)
2. ST elevation
3. Q waves/ Pathological Q waves
4. T wave Inversion
Tombstone Pattern/ Pardee sign ECG
Sinus Arrhythmia ECG
Atrial Fibrillation ECG
Multi-Focal Atrial Tachycardia ECG
Atrial Flutter ECG
Paroxysmal Supraventricular Tachycardia ECG
Wolf Parkinson White (WPW) Syndrome
Hypothermia ECG findings
Ventricular Tachycardia ECG findings
Hyperkalaemia ECG Findings
Bradyarrhythmias ECG Findings
Second-degree Heart Block
Mobitz I or Wenckebach phenomenon
Mobitz II heart block