Infertility Treatment, Causes, Risk factors and Prevention
Jul 7, 2023

Infertility is defined as an inability to conceive even after 1 year of unprotected intercourse. It can further be classified as Primary or Secondary.
- Primary infertility is infertility in a couple who have never been pregnant
- Secondary infertility is infertility in a couple who have a previous child or an abortion
Subfertility is when a couple conceives after trying for almost a year, also called delayed fertility
The chance of Conception with Unprotected Intercourse in 90% of couples is Within 1 year whereas, in 80% of couples, it is Within 1st 6 months. 1 Act of intercourse on the 14th day has a chance of conception of 4-8%. The chance of conception with multiple acts in one month is 25%.
Fecundability is the probability of having a pregnancy in one cycle/ number of cycles taken to conceive whereas Fecundityis the ability to have a live birth.
Read this blog further to get a quick overview of this important topic for OBSTETRICS AND GYNECOLOGY to ace your NEET PG exam preparation.
Causes of Infertility
Every step must be successfully performed for ovulation and fertilization to occur as intended. There are many potential causes of infertility, some of which may even be present at birth.
The causes of infertility may impact both partners or only one. There is seldom a consistent cause.
The percentage of the distribution of cases responsible for infertility is as follows:
- Male→ 20-30%
- Female→ 30-40%
- Males + Females → 10-40%
- Unexplained→ 10-20%
Causes of Male Infertility
- Oligospermia
- Azoospermia
- Psychiatric disorders like erectile dysfunction, premature ejaculation
Causes of Female Infertility
- Anovulatory factors are most common followed by Tubal factors. Anovulation is also the most treatable cause.
Who Classification of Anovulation
- Type I: Hypogonadotropic Hypogonadism: (10%)
- Low LH, FSH
- Central cause
- Sheehan syndrome, Kallman’s syndrome
- Type II: Normogonadotropic Hypogonadism (MC: 85%)
- Most common
- Normal LH, FSH (ratios may be abnormal)
- PCOD
- Type III: Hypogonadotropic Hypogonadism
- High LH, FSH
- Premature ovarian failure → low estrogen → no feedback to brain → High LH, FSH
- Type IV: Hyperprolactinemia)
Risk Factors Of Infertility
The risk factors for male and female infertility share many similarities. They comprise
- Age- Age-related losses in women's fertility occur gradually, with a sharper decline occurring after the age of 37, especially in the mid-30s. Older women's infertility is probably caused by their eggs being of decreased quality and quantity, while it is possible that it is also a result of fertility-related health issues.
- Use of tobacco- Both partners' use of tobacco or marijuana may lessen the likelihood of conception. Smoking also decreases the potential efficacy of reproductive treatments. Women who smoke have a higher rate of miscarriages. Smoking can make men more susceptible to erectile dysfunction and poor sperm counts.
- Use of alcohol- There is no safe level of alcohol consumption for women during conception or pregnancy. Infertility and alcohol usage may go hand in hand. Heavy drinking among men might reduce sperm count and motility.
- Having a weight issue- A sedentary lifestyle and being overweight may raise the risk of infertility in American women. Being overweight may also have an impact on sperm count in men.
- Being underweight- Women who have eating disorders, such as anorexia or bulimia, or who adhere to an extremely low-calorie or restrictive diet are particularly vulnerable to issues with infertility.
- Exercise problems. Obesity raises the chance of infertility because obesity is a result of insufficient exercise. Less frequently, women who are not overweight and who engage in frequent, intensive, severe exercise may experience ovulation issues.
Diagnosis Of Infertility
Prior to doing infertility tests, your doctor or clinic tries to understand your sexual behavior and could offer suggestions to increase your chances of becoming pregnant. Unexplained infertility refers to cases of infertility in which there is no clear reason.
Male fertility depends on the testicles producing enough healthy sperm and on the sperm traveling to the egg successfully when they ejaculate into the vagina. Tests for male infertility try to see if any of these processes are impaired.
You might undergo a general physical examination that includes a genital exam. Specific fertility tests might include:
- Semen examination- more than one semen sample can be required for this procedure. Typically, getting semen involves halting a sexual encounter and ejaculating semen into a clean receptacle. In a lab, a semen sample is analyzed. In some cases, it may be possible to test for sperm in urine.
- Hormone analysis. to measure testosterone levels
- Genetic examination. Genetic testing may be carried out to determine whether a genetic anomaly is the cause of infertility.
- An examination of the prostate. In some cases, a testicular biopsy may be performed to look for defects causing infertility or to obtain sperm for IVF or other assisted reproductive techniques.
- Imaging- Under some conditions, imaging procedures like vasography, transrectal or scrotal ultrasounds, or brain MRIs may be performed.
- Extra specific tests- In unusual cases, other sperm quality tests may be performed, such as examining a sample of semen for DNA abnormalities.
Female
Women's fertility depends on their ovaries producing healthy eggs. In order to be fertilized, an egg must be able to travel through the reproductive system and into the fallopian tubes. The fertilized egg needs to get there in order to implant in the uterine lining. Finding out if any of these systems are compromised is the goal of tests for female infertility.
A routine gynecological exam could be part of your standard physical examination. Particular fertility testing could consist of:
- TVS
- Ovulation tests
- Basal body temperature is more than 0.5° F as Progesterone is thermogenic, hence a rise in basal body temperature is suggestive retrospectively of ovulation
- Serum Progesterone of more than 3ng/ml on day 21, is retrospectively suggestive of ovulation
- LH: more than 15 IU
- Serial USG - Follicular Monitoring is done serially from day 9 onwards, to follow the growth and rupture of a dominant follicle. This is the most common method used.
- Direct evidence is by laparoscopy, a yellow puncta on the ovary is suggestive of ovulation.
- Cervical mucous studies: Loss of spinnbarkeit and ferning due to progesterone. Note that the presence of both of these is suggestive of estrogen effect and not ovulation.
- Premenstrual Endometrial biopsy: This is done from day 20-26, in the premenstrual period. The presence of Secretory changes is suggestive of ovulation. Endometrial changes should correspond to the day of the biopsy, thus when the difference b/w observed & expected changes are of more than 2 days, it implies Luteal Phase Defects, which are an important cause of infertility.
- Mittelschmerz: Mid-cycle pain, however, is not a very reliable sign of ovulation
- Hysterosalpingography- A radio-opaque dye is pushed into the uterus with a Leech cannula, and the uterine cavity and tubes are seen with fluoroscopy. It outlines both uterine cavity and tubal patency. However, it does not tell about outer adhesions/ endometriosis
- Sonosalpingography: Fluid is pushed into the cavity and the outline is thus better seen on USG
- Laparo Hysteroscopy- It is a better investigation to know the anatomy, adhesions, and endometriosis affecting fertility. Along with this, the dye can be put through the cervix, which can be seen coming out of the tube through the laparoscope, known as chromopertubation, which confirms tubal patency.
In the same sitting, a hysteroscopy is done to check the uterine cavity for anatomical defects or lesions, or adhesions. If an HSG is done, which shows blocked tubes, a laparoscopy must be done to confirm.
Treatment of Infertility
1. Ovulation Induction
- Indicated for anovulation and also for timing of intercourse in ovulating women
- In PCOS, high estrogen from multiple small follicles inhibits the hypothalamus, which inhibits the production of gonadotropins, thus drugs used for ovulation involve, inhibition of this negative feedback on the hypothalamus to make Gonadotropins and cause follicle development and ovulation.
- Clomiphene citrate- It Blocks the hypothalamic estrogen receptor to inhibit negative feedback from estrogens, thus increasing FSH. The dose used is 50-250 mg/day from day 2-6 + follicle monitoring. 80% of women will ovulate with clomiphene while 40% will conceive
- Letrozole- It is an aromatase inhibitor that inhibits peripheral conversion of androgens to estrogens, less estrogen thus causing less negative feedback inhibition of the hypothalamus, making more FSH, thus more follicle development.
The dose used is 2.5-5 mg/day, given from days 2-6. This is the drug of choice for ovulation induction
- Inj FSH
- Inj HMG (human menopausal gonadotropin: LH + FSH)
2. IntraUterine Insemination
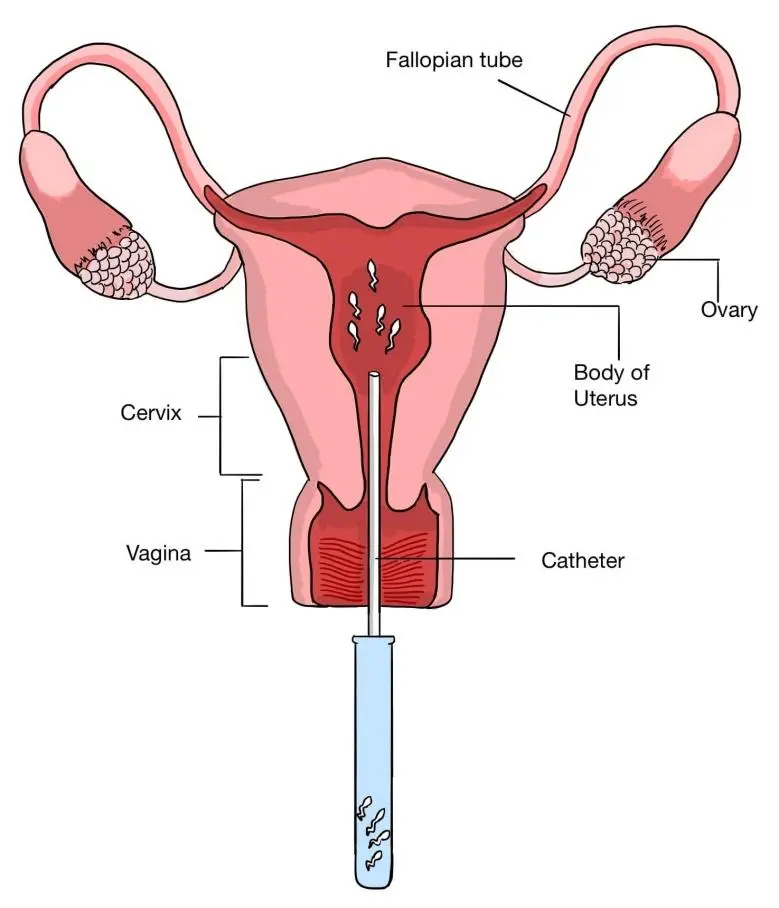
Artificial insemination of prepared semen into the uterine cavity is called IUI. Indications are:
- Cervical factor like stenosis, anti-sperm antibodies
- Endometriosis
- Low sperm counts: 5-10 million
This ovum is prepared by ovulation induction and washed sperm are placed in the uterine cavity by an IUI cannula at the time of ovulation. Note that SEMEN directly is never placed in the uterine cavity. The success rate is around 20-25%
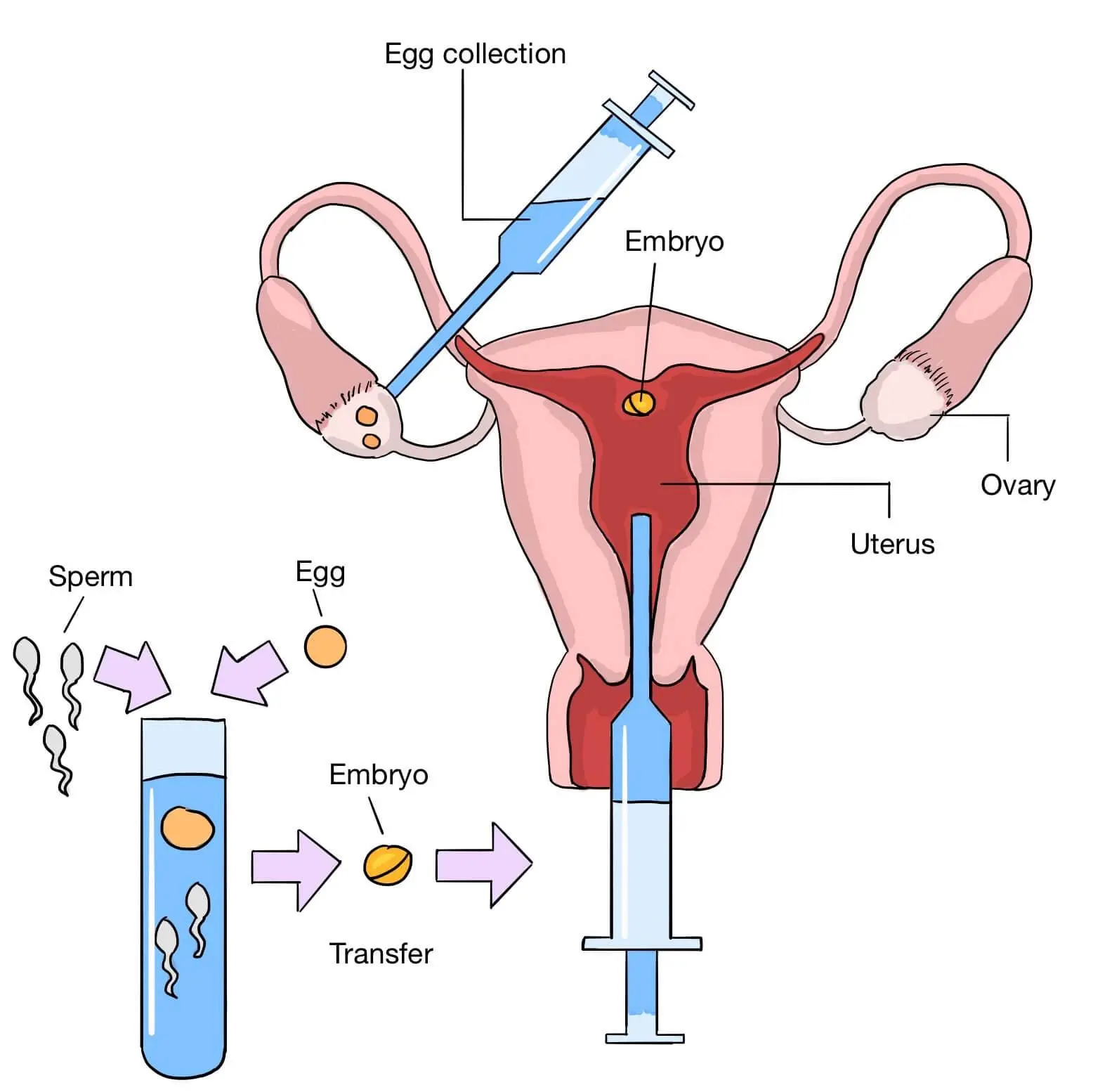
3. In Vitro Fertilization
High-dose ovulation induction is done to cause superovulation which recruits around 6-15 eggs. Retrieved oocytes by transvaginal aspiration are Fertilized in test tubes. In 2 or 3 Day 3 (8 cells) embryos are transferred or 1 or 2 Day 5 (Blastocysts) embryos are transferred.
Indications
- All indications of IUI +
- Tubal blockage
- Sperms required: at least 3-5 million
- Success rate: 45%
Invitro Fertilization
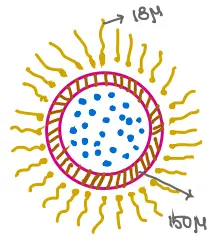
- In normal intercourse, most sperms die due to vaginal acidity and much less reach progressively up till oocyte. Around 1/5th of semen will ultimately reach the site of fertilization. Around 1 lakh sperms now collide with ovum & release Acrosin (like hyaluronidase). This acrosin softens the Zona Pellucida known as Acrosome Reaction. One sperm now enters the ovum and fertilization occurs. This is followed by Cortical Reaction, which again, prevents Polyspermy.
- Capacitation: loss of cholesterol/ Ca influx/ tyrosine phosphorylation: this is a process by which a sperm becomes capable to fertilize, occurs in Cervical Mucus/ Proximal Fallopian Tube (better answer Proximal Fallopian Tube)
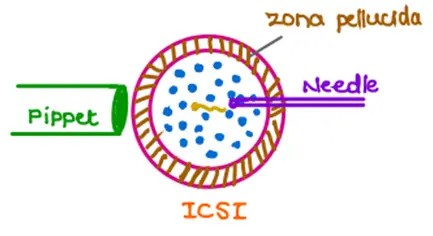
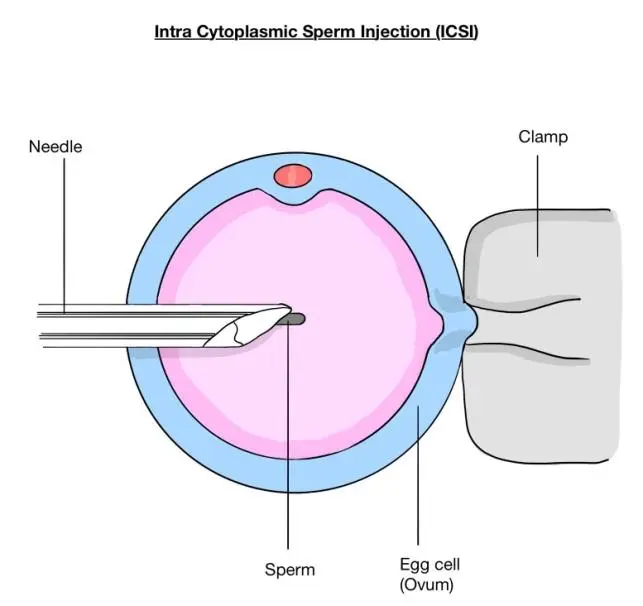
4. IntraCytoplasmic Sperm Injection
- Indicated for very low sperm count < 1 million
A tiny needle, called a micropipette, is used to inject a single sperm into the center of the egg. Once fertilization occurs, the embryo grows in vitro for 1 to 5 days before it is transferred to the uterus.
Azoospermia
- For spermatogenesis, the hypothalamus releases FSH, which acts on the testes to produce sperms and androgens. These androgens give negative feedback which regulates FSH.
- Central cause (pretesticular) Hypothalamic/ kallmans: It is characterized by Low FSH, LH
- Testicular cause: Mumps orchitis, etc. Here, there is no androgen production from the testes, thus no negative feedback, thus high FSH, and LH.
- Post testicular (Obstructive) azoospermia: Vas obstruction. Here there are normal levels of LH, FSH, and Androgens. In any male with normal FSH & azoospermia on semen analysis, think of obstructive azoospermia.
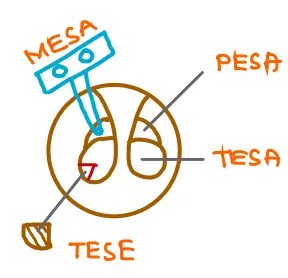
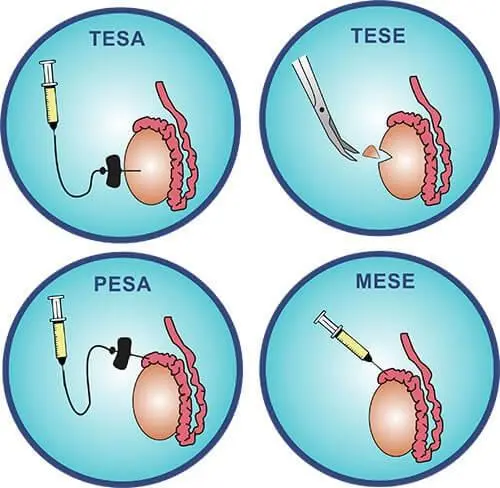
Sperm Extraction Techniques
- For obstructive azoospermia
- PESA [Percutaneous Epididymal Sperm Aspiration]
- TESA [Testicular Sperm Aspiration]
- MESA [ Microsurgical Epididymal Sperm Aspiration]
- TESE [Testicular Sperm Extraction]
.jpg)
Complications of Treatment of Infertility
Complications from infertility therapy could include the following:
- Multiple pregnancies, many pregnancies. Multiple pregnancies, including twins, triplets, and more, are the most frequent side effects of infertility treatment. Preterm labor and delivery, as well as pregnancy issues like gestational diabetes, are often made more likely by the number of fetuses. Premature birth increases the risk of developmental and medical issues in the child. Before beginning treatment, talk with your doctor about any worries you might have regarding a multiple pregnancy.
- Ovarian hyperstimulation syndrome- When combined with ART, ovulation-inducing fertility drugs can result in OHSS, a painful enlargement of the ovaries. Other signs and symptoms include little nausea, bloating, and minor abdominal pain that lasts for about a week—or longer if you have a weakened immune system. Rarely, a more serious variant can result in fast weight gain, shortness of breath, and the need for emergency care.
Also Read : Urethritis: Causes, Symptoms, Types, Diagnosis, Treatment, Complications and Prevention
Prevention Of Infertility
Some types of infertility cannot be prevented. However, a few tactics could improve your chances of getting pregnant.
Couples
For the highest pregnancy rate, engage in regular sexual activity many times around ovulation. Your chances of getting pregnant increase if you have sexual contact starting at least five days before ovulation and continuing until the next day following. For most women with menstrual cycles that are around 28 days apart, ovulation often happens in the middle of the cycle, or halfway between periods.
Men
Although the majority of male infertility issues cannot be avoided, the following measures might be helpful:
- Avoid using drugs, smoking, and consuming excessive amounts of alcohol because these behaviors may increase the risk of male infertility.
- Avoid using hot tubs and hot baths since they can temporarily impair sperm motility and production.
- The generation of sperm can be impacted by exposure to industrial or environmental pollutants.
- Prescription and over-the-counter pharmaceuticals should both be avoided if they may affect fertility. Don't discontinue taking prescription drugs without consulting a doctor; instead, discuss any medications you frequently take with your doctor.
- Mild exercise is advised. The likelihood of becoming pregnant may rise as a result of regular exercise improving sperm quality.
Women
Several tactics for women may improve their chances of getting pregnant, including
- Don't smoke- In addition to harming your overall health as well as the health of a fetus, tobacco use has various detrimental impacts on fertility. Quit smoking immediately if you plan to become pregnant.
- Avoid the use of alcohol and illegal drugs. Your chances of getting pregnant and having a healthy baby may be hampered by these chemicals.
If you're attempting to get pregnant, avoid alcohol use and recreational drugs like marijuana.
- Caffeine Intake- - the intake should be moderate. Caffeine use should be restricted for women who are attempting to get pregnant. To take caffeine safely, seek advice from your doctor.
- Mild exercise is advised. Regular exercise is good, but exercising so hard that your periods become irregular or nonexistent can impact fertility.
- Being overweight- The ability to conceive may be hampered by being overweight or underweight.
To scale up your NEET PG preparation with the best-in-class video lectures, QBank, Mock Tests, and more, download the PrepLadder App!
Download PrepLadder's NEET PG preparation app for Android
Download PrepLadder's NEET PG preparation app for iOS

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Causes of Infertility
Causes of Male Infertility
Causes of Female Infertility
Risk Factors Of Infertility
Diagnosis Of Infertility
Female
Treatment of Infertility
1. Ovulation Induction
2. IntraUterine Insemination
3. In Vitro Fertilization
4. IntraCytoplasmic Sperm Injection
Complications of Treatment of Infertility
Prevention Of Infertility
Couples
Men
Women
Top searching words
The most popular search terms used by aspirants
- Gynecology OBGYN
- NEET PG OBGYN
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial