Molar Pregnancy and Gestational Trophoblastic Disease - NEET PG OBGYN
Feb 15, 2023

Molar pregnancy is an important topic for the NEET PG exam because it is a rare but serious type of gestational trophoblastic disease (GTD) that can have significant implications for the health of the mother and the developing fetus.
In the NEET PG exam, questions related to molar pregnancy can be included in the obstetrics and gynecology section and can test a candidate's knowledge and ability to diagnose and manage gestational trophoblastic diseases.
Read this blog further to get a quick overview of this important obstetrics and gynecology topic for NEET PG exam preparation.

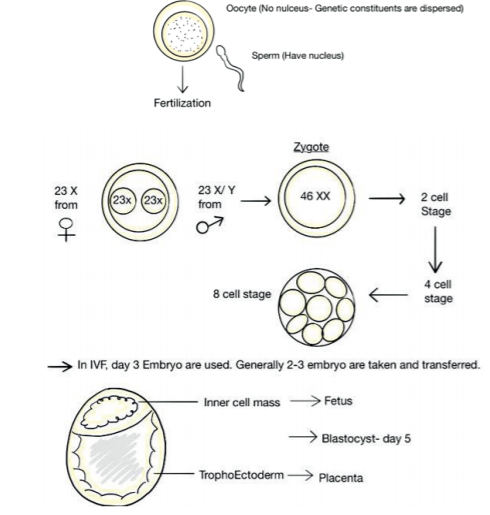
Normal Reproduction
Pathogenesis of molar pregnancy
- Formation of partial mole: If Oocyte is fertilized by 2 sperms
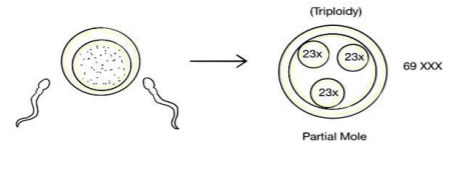
- Partial Mole
- Fetus that is partly degenerated by vesicles.
- It causes Choriocarcinoma in only 2-3% cases (almost not seen)
- Better prognosis than complete mole.
- It can also be, 69XXX (mainly), 69XYY, 69 XXY and can never be 69 YYY
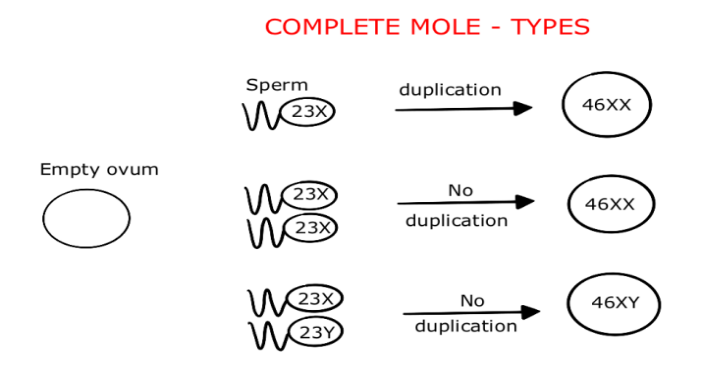
- Complete mole
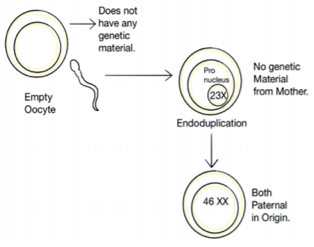
- It can be 46 XX (mainly), 46 XY and can never be 46 YY.
- The degenerated villi formation occurs: Start imbibing fluid and numerous vesicles appear
- There is 20% risk of choriocarcinoma.
- Aborts by itself (12- 16 week)
- Difference between partial and complete mole
|
Complete mole |
Partial mole |
|
|
Pathology |
||
|
Fetal or embryonic tissue |
Absent |
Present |
|
Hydropic Swelling of villus |
Diffuse |
Focal |
|
Trophoblastic hyperplasia |
Diffuse |
Focal |
|
Implantation site trophoblast |
Marked atypia |
Mild atypia |
|
Karyotype |
46 XX (mainly), 46 XY |
Triploid (69XXX) |
Presentation of complete mole
- M / C: Bleeding
- ↑↑ BP
- Hyperthyroidism as HCG acts similar to TSH
- Rarely passage of grape like vesicles (rare)
- Uterine size > POG
- Hyperemesis (due to HCG ↑)
Mx of complete mole
- Any size: Suction / Evacuation, followed by check curettage (after 1 week) because there might be retained bits
- Chest X-ray because it is M / C site of Mets
- HCG values: Should be followed for at least 6 months after it comes negative
- HCG comes negative in 9 weeks: Complete mole
- HCG comes negative in 7 weeks: Partial mole
| Important Information In the follow up period of 6 months, there should not be any pregnancy and we give contraception. |
.jpg)
Gestational Trophoblastic Neoplasia
- Persistence of Trophoblastic tissue is confirmed by
- Continuous bleeding occurs
- High HCG >100000
- Persistently ↑↑ HCG ± 10% of previous value
- Bulky / Enlarged uterus
- If there is confusion at HPE of Complete Mole or partial Mole: P57 KiP 2 immune staining is done; P57 in immune staining only seen with maternal contribution in the Karyotype, in partial mole
- Complete mole will not show P57 KiP2 staining.
- High Risk of Choriocarcinoma is seen with
- HCG > 105
- Very large uterus
- Theca Lutein cysts (high HCG) > 6cm size
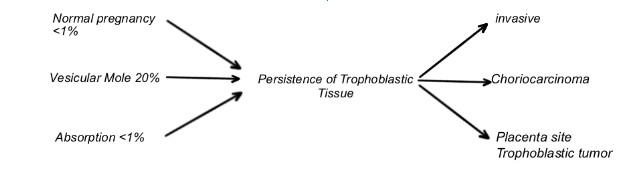
- Invasive mole
- Does not follow normal pregnancy
- Marker: HCG
- Surgery is mainstay of treatment
- Choriocarcinoma
- Marker: HCG
- Chemotherapy is treatment of choice
- For older women hysterectomy can be done
- Placental site trophoblastic tumor
- Marker: HPL (from cytotrophoblast, and its derivative intermediate trophoblast)
- Hysterectomy is best management
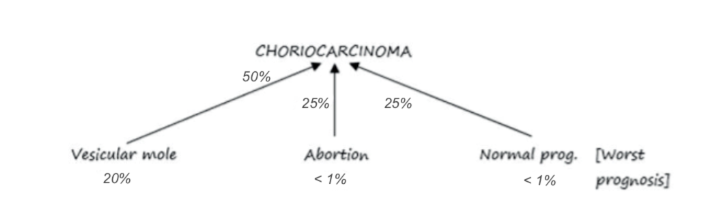
Choriocarcinoma
- WHO classification for risk assessment/prognosis
| Risk factor | 0 | 1 | 2 | 4 |
| Age | = 39 | > 39 | ||
| Antecedent pregnancy | Hydatidiform Mole | Abortion | Term | |
| Interval (months) from antecedent pregnancy | <4 | 4 to 6 | 7 to 12 | > 12 |
| Human chorionic gonadotropin (HCG) (IU/L)6 | <103 | -104 | -105 | >105 |
| ABO blood group (female x male) | 0 x A A x 0 | AB | B | |
| Largest tumor mass, including uterine (cm) | 3-5 | >5 | ||
| Site of Metastases Number of metastases | Spleen 1-4 | GI tract 5-8 | Brain > 8 | |
| Prior chemotherapy | Single drug | Two or more |
- WHO classification was used earlier, which includes blood groups also.
- But now it has been replaced by FIGO classification, which says blood group is not considered as a risk factor
- FIGO Scoring
| FIGO Scoring | 0 | 1 | 2 | 4 |
| Age (years) | <40 | ≥40 | - | - |
| Antecedent pregnancy | Mole | Abortion | Term | |
| Interval months from end of index pregnancy to treatment | <4 | 4 to <7 | 7 to <13 | ≥13 |
| Pretreatment serum hCG (IU/l) | < 10 3 | 10 3 to <10 4 | 10 4 to <10 5 | ≥ 105 |
| Largest tumour size, including uterus (cm) | < 3 | 3 to < 5 | ≥5 | - |
| Site of metastases | Lung | Spleen, kidney | Gastro intestinal | Liver, brain |
| Number of metastases | 1-4 | 5-8 | >8 | |
| Previous failed chemotherapy | Single drug | 2 or more drugs |
- Low Risk score <7
- High Risk score ≥ 8
- Staging of trophoblastic Disease (Choriocarcinoma)
| Stage | Site of Metastasis | Prognosis | Management |
| I | Uterus | Good | Single Agent Chemo |
| II | Pelvis | Based on scoring | if Low score: Single agent chemoIf High score: Multi agent chemo |
| III | Lung metastasis | Based on scoring | If Low score: Single agent chemoIf High score: Multi agent chemo |
| IV | Distant Metastasis | Poor | Multi agent chemo is used |
- MC site of metastasis is lungs
- 2nd MC site of metastasis: Vagina (sub urethral nodule): This appears as a bluish spot in the vaginal area and if you take biopsy of this area, severe hemorrhage can occur, which cannot be controlled by suturing & urgent Radiotherapy needs to be given to control it.
Also Read:
Vaginal Yeast Infections: Causes, Symptoms, Risk Factors, Diagnosis, Treatment and Complications
Postpartum Hemorrhage: Causes, Types and Management
Genital Warts: Causes, Symptoms, Risk Factors, Diagnosis, Treatment and Complications
Previous Year Questions
Q. Patient with 10 weeks of amenorrhea, size of uterus 12 to 14 weeks, with severe nausea and vomiting, snow storm appearance on ultrasound, management? (AIIMS 2020)
A. Follow up with hCG levels
B. Continue pregnancy
C. Suction and Evacuation
D. Diagnostic Laparoscopy
Exciting news! We're now offering OBS-GYN Residency preparation course to empower doctors with detailed clinical knowledge. Curated by India's top OBS-GYN faculty, Dr. Shonali Chandra, our program features 200+ hours of video lectures covering high-yield topics from the last 10 years. Engage in clinical case discussions within lectures to enhance your diagnostic skills. Join us in preparing for OBS-GYN Residency and advancing your expertise in obstetrics and gynecology.
To study this topic in detail, download the PrepLadder app and get access to engaging video lectures, self-explanatory notes and MCQs covering the topic.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!