Neonatal Jaundice Breast Milk Jaundice, Phototherapy
Feb 16, 2023

Neonatal jaundice is an important topic for the NEET PG exam in pediatrics as it is a common condition affecting over 60% of newborns and is a leading cause of hospital readmission in the first 2 weeks of life.
Jaundice in newborns can be a sign of underlying diseases such as hemolytic anemia, infection, or liver dysfunction, and early recognition and treatment are essential to prevent severe complications such as kernicterus, which can lead to permanent brain damage.
Let's learn about this commonly tested topic in the NEET PG exam.
Overview
Clinical jaundice in neonates: At bilirubin level >5 mg / dL. Very common in neonates
|
Physiological jaundice |
Pathological jaundice |
|
|
|
|
|
|
|
|
Breastfeeding jaundice
- It is due to inadequate breastfeeding
- Rx: Adequate & frequent breastfeeding
Breast milk jaundice
- Jaundice due to certain substances present in breast milk like pregnanediol or FFA that interferes with conjugation of bilirubin. Breastfeeding should be continued, it is withheld only when bilirubin level goes >20 mg/dL
|
Etiology of unconjugated hyperbilirubinemia |
|
|
Increased production bilirubin |
Decreased conjugated of bilirubin |
|
|
- Conjugated hyperbilirubinemia: When level of conjugated bilirubin >2 mg /dL or >20% of total bilirubin
|
Etiology of conjugated hyperbilirubinemia |
|||||
|
Non obstructive |
Obstructive |
||||
|
|
||||
- For diagnosis of EHBA: Screening test of choice is HIDA scan
- Surgery of choice: Kasai procedure
- Good prognosis, if procedure is done at <8 weeks of age
- Bad prognosis, if procedure is done at >8 weeks of age
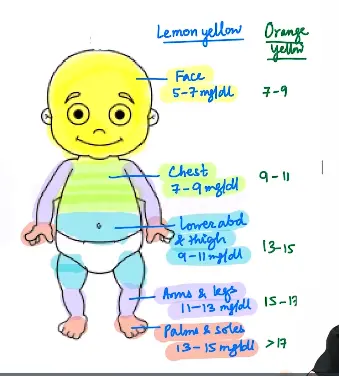
Clinical assessment of Neonatal Jaundice
- Done by Modified Kramer’s rule. Jaundice in neonates have cephalocaudal progression
- Not reliable in preterm babies or neonates who have already received phototherapy - Transcutaneous bilirubinometer or serum bilirubin is done in those cases.
Kernicterus (CNS manifestation of Hyperbilirubinemia)
- Part of the brain most commonly involved: Basal ganglia. Type of cerebral palsy most commonly seen due to neonatal jaundice: Extrapyramidal type
- Features of Acute Bilirubin encephalopathy
- Early stages: Hypotonia, lethargy, poor feeding
- Late stages: Hypertonia, Fever, Opisthotonic Posture, Coma, Seizures & Death
- Features of chronic bilirubin encephalopathy: SADMUM
- SNHL
- Athetosis
- Dental enamel changes
- Mental Retardation
- Upward gaze palsy
- Rx:
- Phototherapy
- Exchange transfusion in cases of severe jaundice
- IvIg - In case of Erythroblastosis fetalis
Phototherapy
- Most effective wavelength of light: 460-490 nm. Most important mechanism: Structural isomerisation
- Other methods:
- Photoisomerization
- Photo oxidation
- Minimum irradiance recommended: 30 µW/ cm2/ nm. Measured by lux meter
- Ways to increase the effectiveness of phototherapy
- Increase exposed surface area of baby
- Decrease distance between baby & phototherapy unit
- Use of LED lights
- Adverse effects of phototherapy - Skin colour of baby becomes darker therefore called as bronze baby syndrome
- Watery diarrhoea
- Dehydration
- Hypocalcemia
- Retinal toxicity
- Gonadal toxicity / mutation
- Impaired maternal child bonding
- Indication of phototherapy in a neonate
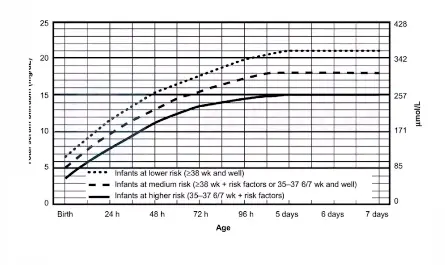
- Cut off levels in otherwise healthy term babies.
| Age | For phototherapy | For exchange transfusion |
| 24-48 hrs of life | >15 mg /dl | >20 mg/dl |
| 48-72 hrs | >18 mg /dl | >25 mg /dL |
| >72 hrs | >20 mg/dL | >25mg/dL |
| Preterm babies | 1% of birth weight (in gm) | PT cut off +5 |
- Indication of exchange transfusion in neonates with Rh incompatibility done if cord blood bilirubin is - >5 mg/dL, Cord blood Hg - <10 gm/dL
- Most common cause of neonatal mortality in India:
- Prematurity & related complications: M/C
- Sepsis
- Birth asphyxia & birth trauma
- Congenital abnormalities
- Common cause of Under-5 mortality in India:
- Prematurity related complications: M/C
- Pneumonia
- Diarrhea
- Injuries
- Malaria
To learn more about this topic and other high-yield topics from Pediatrics, download the PrepLadder app and find engaging video lectures covering the topic in detail.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Overview
Breastfeeding jaundice
Breast milk jaundice
Clinical assessment of Neonatal Jaundice
Kernicterus (CNS manifestation of Hyperbilirubinemia)
Phototherapy
Top searching words
The most popular search terms used by aspirants
- neet pg pediatrics
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial