High-Yield Psychiatry Topics for NEET PG 2026: Key Disorders, Drugs & MCQ Pearls
Apr 7, 2026
A 28-year-old guy ends up in the ER after police found him wandering and talking to himself. He is absolutely convinced that government agencies are tracking his thoughts through radio waves. He hasn’t been taking care of himself, and he doesn’t show much emotion. His drug screen comes back clean. So, what’s going on with him? What do you think is the diagnosis? Spoiler- It's probably schizophrenia. Psychiatry questions like this show up a lot in NEET PG. If you know what to look for, you can score high.
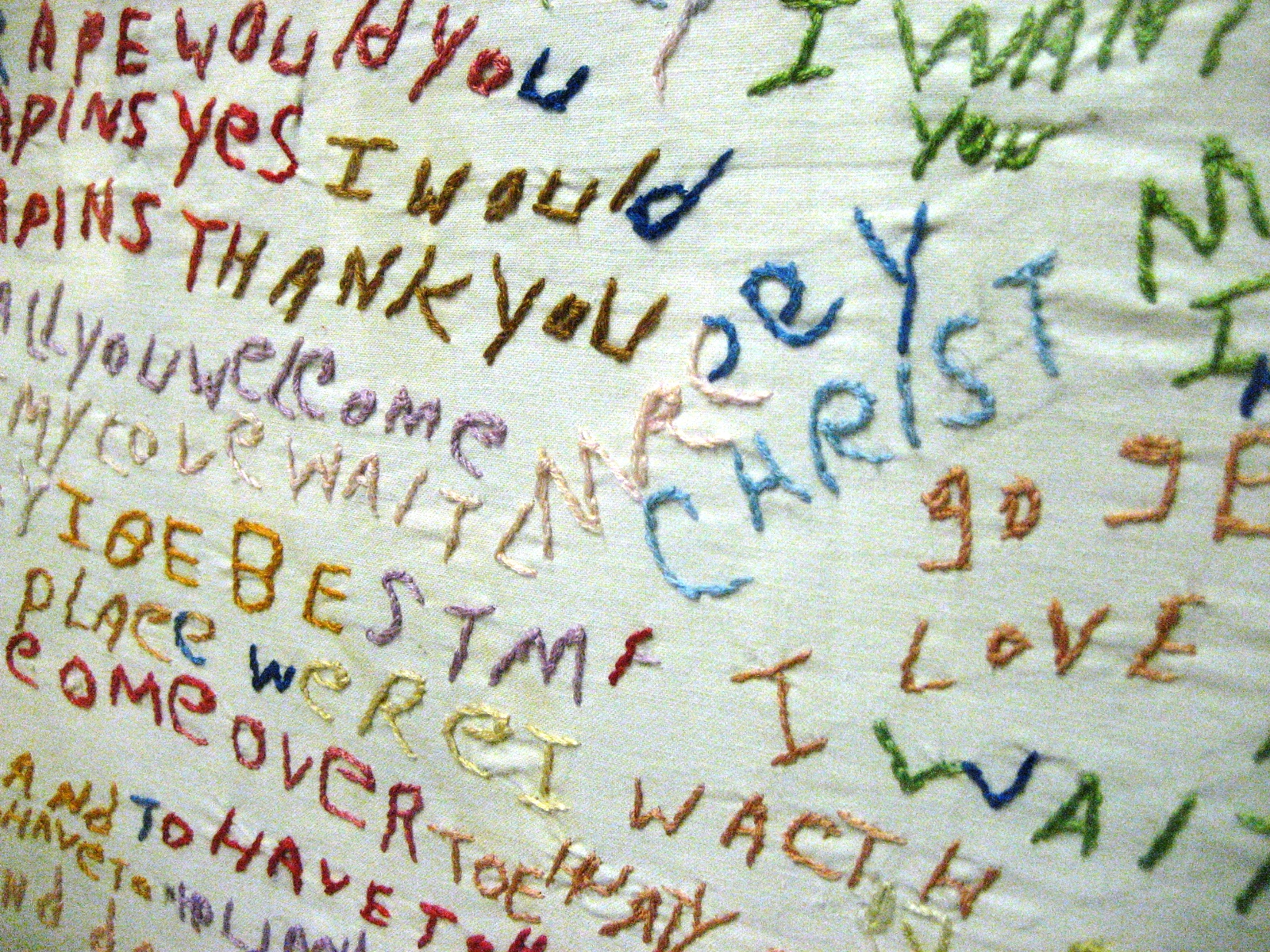
A schizophrenic patient made this textile art, which is now showcased at the Glore Psychiatric Museum.
Let's talk: Psychiatry pops up a lot in NEET PG. On an average day, you’ll see 8-12 questions on the exam paper.
- The most important areas?
- Schizophrenia (especially the dopamine hypothesis and those famous first-rank symptoms). It tends to show up in 2 to 3 questions each time.
- Mood disorders (think drug therapy and everything about lithium)
- Anxiety disorders like OCD and PTSD
- Lately, examiners are leaning into side effects of psych meds, plus DSM-5-TR diagnostic criteria.
You can’t really afford to ignore psychiatry-it’s high-yield and never goes out of style on the exam.
In This Post, you’ll read:
- Why psychiatry often gives you easy marks
- Schizophrenia - the single most important topic
- Mood Disorders - depression and bipolar disorder
- Anxiety Spectrum - OCD, PTSD & Panic Disorder
- How to differentiate between delirium and dementia
- Psychopharmacology
- Substance Use Disorders - Alcohol & Opioids
- Quick reference: Psychiatric Emergencies
- High-Yield Points for NEET PG
- FAQs
Why Psychiatry often gives you Easy Marks.
In NEET PG psychiatry, recognising patterns is more important than memorising facts.
- In our 11 years of service in guiding NEET PG aspirants, we've seen students get 6 to 10 extra points just by learning 5-6 basic psychiatric topics.
- You can guess how the questions will be asked.
- Examiners consistently evaluate identical diagnostic criteria, drug side effects, and clinical vignettes.
- Psychiatric presentations on the wards significantly overlap with Medicine and Pharmacology.
- For example, a question about serotonin syndrome tests your knowledge of psychiatry, pharmacology, and emergency medicine all at once. Because it can be used in so many different subjects, every hour spent on Psychiatry is very productive.
- Knowing which topics to focus on is the key. Let us show you the specific areas that get the most questions.

Schizophrenia - the single most important topic
Schizophrenia is a persistent psychotic disorder marked by delusions, hallucinations, disorganised thinking, and negative symptoms, enduring for a minimum of six months, including one month of active-phase symptoms as per DSM-5-TR criteria.
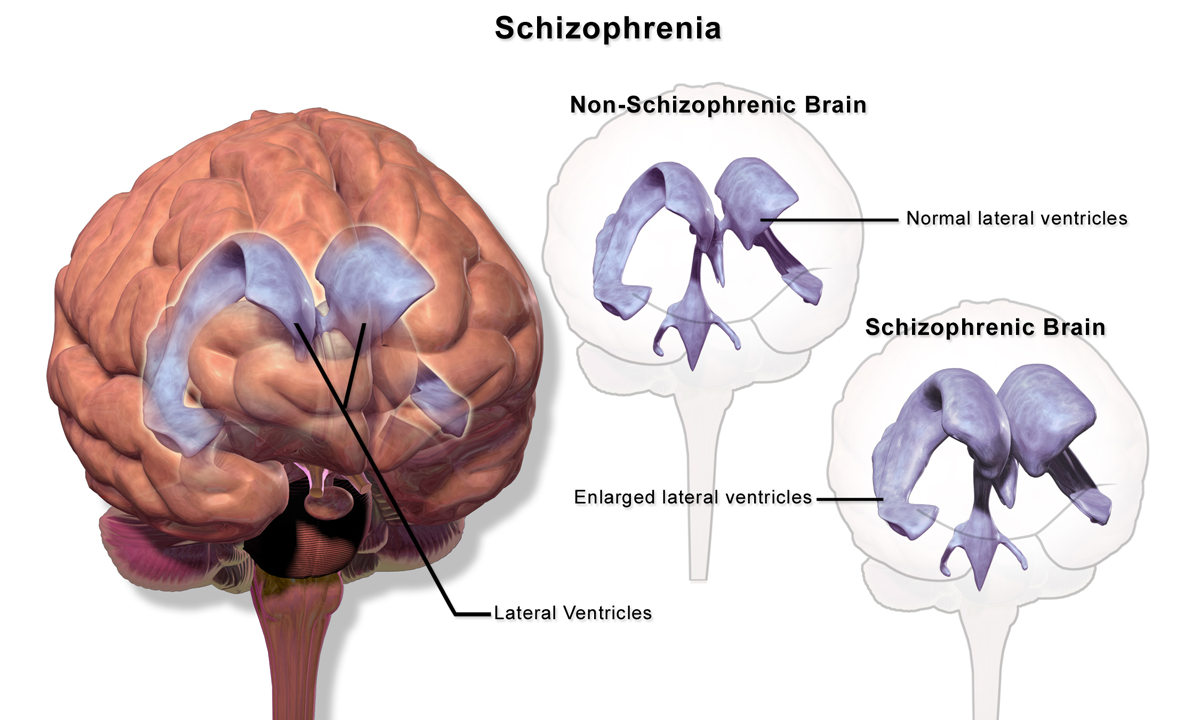
The dopamine hypothesis is still the most tested idea about how the body works.
- It says that hyperactivity of the mesolimbic pathway causes positive symptoms and hypoactivity of the mesocortical pathway causes negative symptoms.
- The mesolimbic pathway is like an "overheating engine" that makes people see things that aren't there and believe things that aren't true.
- The mesocortical pathway is "running cold," which makes people feel apathetic and withdraw from social situations.
What Examiners Test
- First-rank symptoms of Schneider are present in almost every exam cycle.
- Examples of first-rank symptoms include:
- Hallucinations in the third person (i.e., hearing voices),
- Thought withdrawal, thought insertion, thought broadcasting
- Delusional perception.
Basically, in a clinical setting, if you see any question stem stating that the patient hears voices commenting on his actions, then your answer should be schizophrenia until you can prove otherwise.
Treatment:
- Drugs such as clozapine, olanzapine, and risperidone can be used
- Clozapine is the gold standard for treating treatment-resistant schizophrenia, which is defined as having failed at least two adequate antipsychotic trials.
- Side effects of clozapine: The likelihood of producing agranulocytosis (1-2%). Hence, it is important to monitor (i.e., complete blood count) the patient.
- Olanzapine has a greater risk of developing severe metabolic syndrome compared to other atypical antipsychotics.
- Risperidone has a greater tendency to cause elevated prolactin levels than other atypical antipsychotic medications.
- NOTE: For a more in-depth breakdown of antipsychotic pharmacotherapy, please see our guide on psychopharmacology for NEET PG.
Mood Disorders - Depression & Bipolar Disorder
Major Depressive Disorder (MDD) requires at least five symptoms over two weeks, with depressed mood or anhedonia being mandatory.
- The monoamine hypothesis, which blames low levels of serotonin, norepinephrine, and dopamine, is the classic theory you’ll get tested on for NEET PG.
- We’ve noticed a lot of students trip up by mixing up MDD with dysthymia (persistent depressive disorder).
- The difference? Dysthymia hangs around for at least two years but never quite meets the full criteria for MDD. Examiners love to catch people out on this detail!

Tx for Depression:
SSRIs like fluoxetine, sertraline, and escitalopram are your first choice for treating MDD.
- Fluoxetine stands out because it has the longest half-life
- Its active form, norfluoxetine, lasts 2–6 days
- And it’s also the only SSRI cleared for use in children and teens with depression.
One thing you can’t forget for NEET PG: never combine SSRIs with MAOIs.
- That combo leads to serotonin syndrome.
- Which means high fever, muscle clonus, restlessness, and sweating-a dangerous situation examiners expect you to spot.
Tx for Bipolar Disorder:
- Lithium is the first-line for acute mania and prophylaxis.
- The therapeutic window is narrow: 0.6–1.2 mEq/L for maintenance, 1.0–1.5 mEq/L for acute mania.
- Lithium toxicity (>1.5 mEq/L) presents with coarse tremor, ataxia, and renal dysfunction.
- The classic exam trap: lithium is teratogenic (Ebstein's anomaly).
Treatment Algorithm for Acute Mania:
Step 1: Lithium or Valproate (1st line mood stabiliser)
Step 2: Inadequate response → Add an atypical antipsychotic (e.g. Olanzapine, Quetiapine)
Step 3: Refractory case → Electroconvulsive Therapy (ECT - most effective therapy for refractory manic episodes and the first line therapy for treating refractory psychotic depressed states).
Explore mood disorder pharmacology in depth on PrepLadder's Pharmacology section.
Anxiety Spectrum - OCD, PTSD & Panic Disorder
Obsessive-Compulsive Disorder (OCD):
- Cause: Serotonin dysregulation
- 1st line Tx= High dosed SSRIs (Eg, fluoxetine 40-80 mg/day, which is a very high dose compared to patients treated for depression).
- Other Medications: Fluvoxamine and clomipramine
PTSD (Post Traumatic Stress Disorder)
- Cause: Exposure to trauma. It requires symptoms lasting > 1 month.
- 1st line Tx = SSRIs (sertraline and paroxetine are FDA-approved).
- On the wards, prazosin (an alpha-1 blocker) is specifically used for PTSD-related nightmares - a favourite NEET PG question.

Panic Disorder
- Presentation: Recurrent, unexpected panic attacks.
- Alprazolam provides the fastest relief but is not first-line due to dependence risk.
- SSRIs remain the long-term management choice.
- Panic attacks peak at about 10 minutes after onset - this specific timing is frequently tested.
How to differentiate between delirium and dementia
This question has one of the best reliability ratings for comparison questions found in psychiatry; therefore, if you know the table below, then you have obtained at least one point.
| Feature | Delirium | Dementia |
| Onset | Acute (hours to days) | Insidious (months to years) |
| Course | Fluctuating, worse at night (sundowning) | Progressive, relatively stable day-to-day |
| Consciousness | Clouded and impaired | Clear up to the late stages |
| Attention | ||
| Hallucinations | Severely impaired (hallmark) | Relatively well-preserved in early stages |
| Reversibility | Common (Visual) | Less Common (visual in Lewy body dementia) |
| EEG | Reversible if the cause is treated | Irreversible |
| NEET PG pearl | The hallmark symptom of delirium is an inability to attend. | The hallmark symptom of dementia is amnesia. |
.jpg)
Psychopharmacology - Drugs That You Need to Know!
Drug side effects are tested more often than their MOAs. Here are the associations that you need to learn now:
| Drug | High-Yield Side Effect | Additional Exam Pearl |
| Clozapine | Agranulocytosis (1-2%) | Only medication proven effective against treatment-resistant Schizophrenia. |
| Lithium | Hypothyroidism, nephrogenic diabetes insipidus | Ebstein's anomaly in pregnancy; narrow therapeutic index |
| Haloperidol | Neuroleptic Malignant Syndrome (NMS) | High-potency typical → more EPS vs less sedation |
| Chlorpromazine | Blue-grey skin discolouration | Low-potency typical → more sedation vs less EPS |
| Fluoxetine | Longest half-life of all SSRI | Only the SSRI is approved for paediatric depression. |
| Disulfiram | Acetaldehyde syndrome after consuming alcohol. | Aldehyde dehydrogenase inhibitor. |
| NEET PG pearl | NMS vs Serotonin Syndrome differentiation | NMS: "lead-pipe" rigidity, slow onset. SS: clonus, hyperreflexia, rapid onset |
Make sure to practice these MCQ and other related questions with PrepLadder QBank for pharmacology-psychiatry crossover questions.
Substance Use Disorders - Alcohol & Opioids
Alcohol withdrawal has a well-defined timeline that examiners enjoy testing:
- 6 - 24 hours: Anxiety, tremors, and tachycardia
- 12 - 48 hours: Withdrawal seizures (GTCS) are possible.
- 48 - 96 hours: Delirium tremens. The mortality rate when delirium tremens goes untreated is reported to be 5% - 15% (very lethal).
- Treatment:
- Benzodiazepines (chlordiazepoxide or lorazepam)
- Long-term abstinence agents: Maltrexone, acamprosate, and disulfiram.
Opioid overdose presents with the classic triad:
1) miosis (constricted pupils)
2) respiratory depression
3) altered level of consciousness.
Treatment for Opioid Overdose:
- Naloxone acts as the reversal agent and may be given either IV, IM or intranasally.
- Methadone is useful as a long-acting full agonist, while buprenorphine is considered a partial agonist for maintenance therapy.
- Students often confuse naloxone (short-acting and used for reversing an acute overdose) with naltrexone (long-acting; used to prevent relapse). This question is frequently tested on exams.
For the pharmacology of substance use management, see our resource on de-addiction pharmacotherapy.
Comparison Table: Psychiatric Emergencies
Feature Neuroleptic Malignant Syndrome (NMS) Serotonin Syndrome Lithium Toxicity Cause Dopamine blockers (haloperidol, metoclopramide) Serotonergic drugs (SSRIs + MAOIs, tramadol) Serum lithium conc. > 1.5 mEq/L Onset Days to weeks after starting the drug Within 24 hours of changes in the drug Progressive; triggered by dehydration, NSAIDs, and ACE inhibitors Diagnostic hallmark "Lead-pipe" rigidity, hyperthermia Clonus, hyperreflexia, agitation Tremor, ataxia, seizures Diagnostic test Increased serum CPK (creatine phosphokinase) Clinical diagnosis (Hunter criteria) Serum lithium levels Management Withdrawal of the offending agent + administration of dantrolene and bromocriptine Withdrawal of the serotonergic agent + cyproheptadine Withdrawal of lithium + fluid replacement
Hemodialysis in severe cases NEET PG pearl Rigidity distinguishes NMS from SS Clonus is the most specific finding NSAIDs reduce lithium clearance - a classic exam trap
High-Yield Points for NEET PG
First-rank Schneider’s symptoms are:
- Auditory hallucination in third person,
- Thoughts alienation
- Delusional perception
Management:
- The only antipsychotic drug useful for resistant schizophrenia patients is Clozapine, with CBC monitoring for agranulocytosis
- Lithium:
- Therapeutic range: 0.6-1.2 mEq/L (Maintenance),
- Toxicity: >1.5 mEq/L
- Teratogenic: Ebstein’s anomaly
- Electroconvulsive therapy is the most effective form of treatment for refractory depression, psychotic depression, and catatonia.
- Attention deficit is characteristic of delirium, whereas memory defect is characteristic of dementia.
- Panic attacks reach their peak within 10 minutes - this detail is frequently asked by examiners.
- Alcohol withdrawal seizure occurs after 12-48 hours, and delirium tremens after 48-96 hours
- SHIVERS is a mnemonic for serotonergic syndrome: Shivering, Hyperreflexia, Increased temperature, Vitals instability, Encephalopathy, Restlessness, Sweating.
- The examiner tests for differential diagnosis between NMS and serotonin syndrome.
- Rigidity = NMS,
- Clonus = serotonin syndrome
- Another NEET PG MCQ pitfall - Disulfiram does not decrease craving; rather induces aversion to alcohol through aldehyde dehydrogenase blockade
Practice topic-wise questions in the QBank from the PrepLadder app.
Frequently Asked Questions About Psychiatry for NEET PG
1. What is the most tested psychiatry topic in NEET PG?
Schizophrenia. It contributes to 2-3 questions per paper on average.
- Focus on Schneider's first-rank symptoms, the dopamine hypothesis, and clozapine's role in treatment resistance.
- Antipsychotic side effects are tested almost every year.
2. What is the difference between delirium and dementia?
- Delirium has an acute onset, fluctuating course, and impaired attention as its cardinal feature.
- Dementia has an insidious onset, a progressive course, and memory impairment as the primary deficit.
- Consciousness is clouded in delirium but preserved in early dementia.
3. Which drug is first-line for bipolar disorder?
- Lithium remains the gold standard first-line mood stabiliser for both acute mania and long-term prophylaxis.
- The therapeutic range is 0.6–1.2 mEq/L for maintenance.
- Valproate is an alternative, especially when rapid cycling is present.
4. What is Neuroleptic Malignant Syndrome?
- NMS is a life-threatening reaction to dopamine-blocking agents, characterised by hyperthermia, "lead-pipe" muscular rigidity, altered consciousness, and autonomic instability.
- CPK levels are markedly elevated.
- Treatment involves stopping the offending drug and administering dantrolene and bromocriptine.
5. What causes serotonin syndrome?
- Serotonin syndrome results from excessive serotonergic activity, most commonly from combining SSRIs with MAOIs, tramadol, or linezolid.
- It presents with clonus (the most specific sign), hyperreflexia, agitation, hyperthermia, and diaphoresis.
- Cyproheptadine is the specific antidote.
6. How is psychiatry tested in NEET PG?
- Psychiatry questions in NEET PG are predominantly clinical-vignette-based. Expect a patient scenario followed by a "most likely diagnosis" or "drug of choice" question.
- Psychopharmacology side effects and diagnostic criteria dominate.
- Practising vignette-based MCQs builds the pattern recognition needed to score consistently.

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
Schizophrenia - the single most important topic
What Examiners Test
Mood Disorders - Depression & Bipolar Disorder
Anxiety Spectrum - OCD, PTSD & Panic Disorder
How to differentiate between delirium and dementia
Psychopharmacology - Drugs That You Need to Know!
Substance Use Disorders - Alcohol & Opioids
Comparison Table: Psychiatric Emergencies
High-Yield Points for NEET PG
Frequently Asked Questions About Psychiatry for NEET PG
1. What is the most tested psychiatry topic in NEET PG?
2. What is the difference between delirium and dementia?
3. Which drug is first-line for bipolar disorder?
4. What is Neuroleptic Malignant Syndrome?
5. What causes serotonin syndrome?
6. How is psychiatry tested in NEET PG?
Top searching words
The most popular search terms used by aspirants
- Medical PG Psychiatry
- NEET PG Psychiatry Preparation
- Psychiatry NEET PG