Rapid Revision Reignite Surgery: Question-Answer Format
Sep 9, 2025
Trauma/Shock
Big Question 1: What are the common types of skull base fractures, their clinical features, and how do they differ based on anatomical location?
Broad Answer
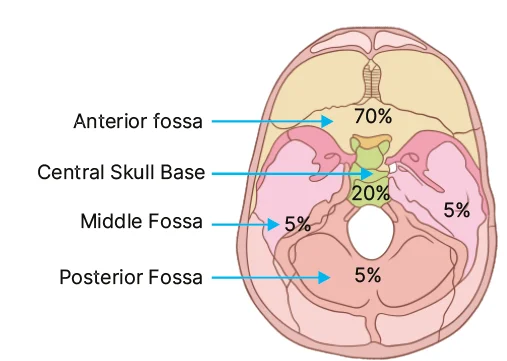
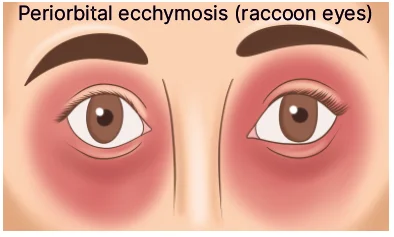
- Anterior cranial fossa fractures are most common (~70%), involving the frontal bone, leading to CSF rhinorrhea, epistaxis, anosmia, raccoon eyes, and frontal lobe contusion.
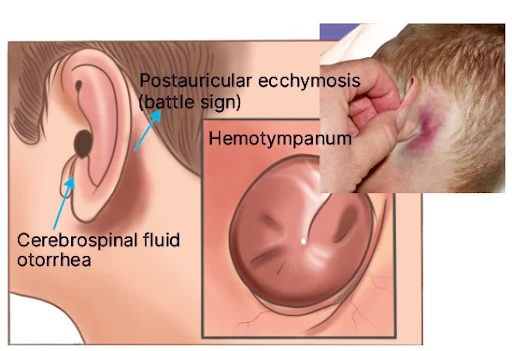
- Middle cranial fossa fractures (~20%) involve the petrous temporal bone, causing CSF otorrhea, Battle sign, VII/VIII CN palsy, and temporal lobe contusion.
- Posterior cranial fossa fractures (~5%) involve the occipital bone, leading to visual disturbances, VI/IX/X/XI CN involvement, and basilar artery injury.
- Diagnosis is clinical and supported by imaging; each site presents with characteristic signs and neurological deficits.
Q1.1: Which is the most common skull base fracture?
Answer: Anterior cranial fossa fracture
Q1.2: What are the incidences of various types of skull base fractures?
Answer:
- Most common: Anterior cranial fossa fracture (70%)
- Middle cranial fossa fracture (20%)
- Posterior cranial fossa fracture (5%)
Q1.3: Describe Anterior cranial fossa fracture
Answer:
- Anterior cranial fossa is mainly composed of frontal bone-fracture leads to frontal lobe contusion
- Mnemonic: Frontal ESCAPe
- Frontal lobe contusion
- Epistaxis
- Subconjunctival hematoma
- SF rhinorrhea
- Anosmia
- PEriorbital hematoma: raccoon eyes
Q1.4: What are the clinical features of a middle cranial fossa fracture?
Answer:
- Middle cranial fossa is mainly composed of temporal bone-fracture leads to temporal lobe contusion
- Fracture of petrous part of temporal bone leads to dural laceration
- Clinical features:
- CSF otorrhea (Tympanic membrane rupture)
- Otorhinorrhea/Paradoxical rhinorrhea (if Tympanic membrane intact)
- Battle sign
- Hemotympanum
- VII, VIII nerve affected
- Temporal lobe contusion
Q1.5: Describe Posterior Cranial Fossa Fracture
Answer:
- Fracture of occipital bone leading to contusion of occipital lobe
- Clinical features
- Visual disturbances
- VI CN injury
- Jugular foramen syndrome (VERNET syndrome): IX, X, XI CN injury
- Basilar artery injury
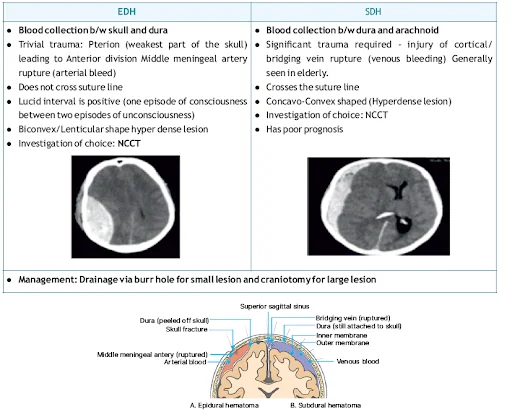
Q1.6: What are the differentiating features of EDH and SDH ?

Facial Injuries And Abnormalities
Big Question 2: What is the classification of midface fractures? Describe their clinical features and significance.
Broad Answer: Midface fractures (Le Fort's) are classified into three types:
Detailed Questions
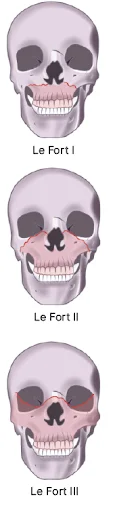
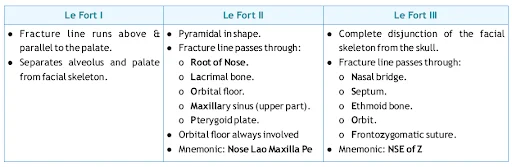
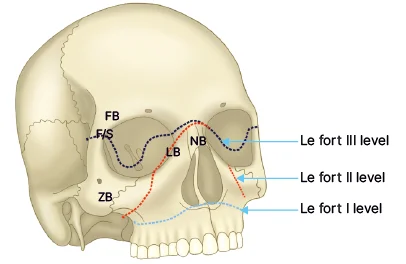
Q2.1: What is the fracture line for a Le Fort I fracture.
Answer: The fracture line runs above & parallel to the palate, separating the alveolus and palate from the facial skeleton.
Q2.2: What is the fracture line for a Le Fort II fracture.
Answer: The fracture is pyramidal in shape and passes through the root of the nose, lacrimal bone, orbital floor, maxillary sinus (upper part), and pterygoid plate. The orbital floor is always involved.
Q2.3: What is the fracture line for a Le Fort III fracture.
Answer: The fracture represents a complete disjunction of the facial skeleton from the skull. The fracture line passes through the nasal bridge, septum, ethmoid bone, orbit, and frontozygomatic suture.
Sutures And Anastomosis
Big Question 3: Compare the different types of surgical knots and suturing techniques used in clinical practice, including their principles and indications.
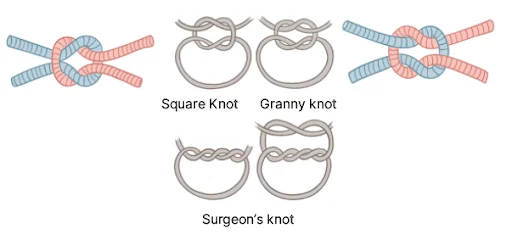
Broad Answer : Surgical knots include the square knot (stable, with crossing in each throw) and the granny knot (less stable, no crossing). The surgeon's knot involves two wraps in the first throw and one in the second to prevent loosening. Simple interrupted sutures are placed at right angles to the incision. Mattress sutures (horizontal or vertical) are used for uneven wound edges. Purse-string sutures are circular and commonly used in herniotomy and appendectomy. For bowel anastomosis, submucosa must be included and the preferred technique is single-layer extramucosal anastomosis with inverted edges to prevent leaks.
Detailed Questions
Q3.1 Describe the different types of surgical knots
Answer:
Square Knot: It is also known as Reef knots
Granny Knot: Granny knot is called pseudo-square knots
Q3.2 What are the similarities between Square knot and Granny knot ?
Answer: There is single wrap in each throw
Q3.3 What are the differences between Square knot and Granny knot ?
Answer:

Q3.4 Describe Surgeon's Knot
Answer:
- Two wraps in the first throw and a single wrap in the second.
- Crossing occurs in each throw.
Q3.5 Describe the technique of a simple interrupted suture.
Answer:
- The needle is inserted at a right angle to the incision.
- Pass through both edges of the wound and exit again at a right angle
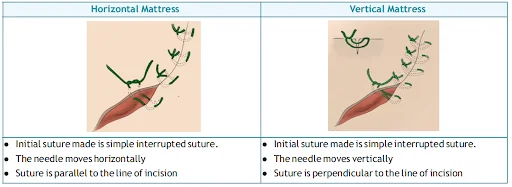
Q3.6 How are mattress sutures used in wound approximation, and what are its types?
Answer:
- Approximation of wound with uneven edges is done by Mattress sutures
- Mattress suture is of two types:
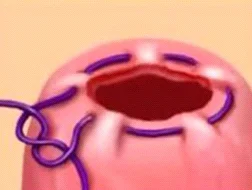
Q3.7 What is a purse-string suture, and where is it commonly used?
Answer:
- In a circular wound, continuous suture is applied parallel to the edges of the circular wound
- It is used in:
- Hernia surgery (Herniotomy)
- Appendectomy
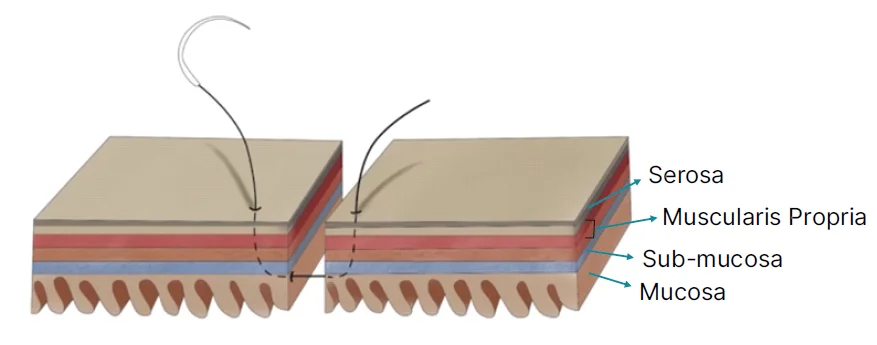
Q3.8 What are the principles of bowel anastomosis ?
Answer:
- The sub-mucosa must be included as it is the strongest layer of the bowel as a result of its high collagen content.
- The edges should be inverted to prevent the risk of a leak.
- Single layer extramucosal anastomosis is the most preferred technique for bowel anastomosis
Arterial Disorders
Big Question 4: What are the causes and clinical manifestations of peripheral arterial occlusion?
Broad Answer: Peripheral arterial occlusion results from sudden or gradual blockage of an artery, most commonly due to thrombus, embolus, or advanced atherosclerosis. This arterial obstruction leads toischemia of the supplied tissues. Clinically, it presents with the classic “5 Ps” (pain, pallor, pulselessness, paresthesia, paralysis) and may vary depending on the site of the occlusion, such as calf, thigh, buttock claudication, or erectile dysfunction in aortoiliac disease.
.jpg)
Detailed Questions
Q4.1: What are the classic clinical features of peripheral arterial occlusion?
Answer:
- The 5 Ps:
- Pain (most common)
- Pallor
- Paralysis
- Pulselessness
- Paresthesia
- Poikilothermia (sometimes added as 6th P)
Q4.2: What is the significance of paralysis and pulselessness in peripheral arterial occlusion?
Answer:
- Paralysis indicates severe ischemia and carries the worst prognosis, especially in compartment syndrome
- Pulselessness is the last feature to develop in compartment syndrome
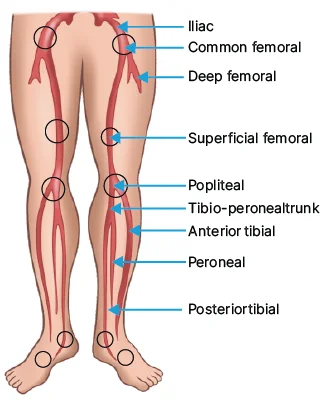
Q4.3: What are the manifestations of aorto-iliac occlusion?
Answer:
- Buttock, thigh, and calf intermittent claudication: Leriche syndrome
- Erectile dysfunction - Impotence
Q4.4: Which sites of arterial obstruction cause calf claudication?
Answer:
- Superficial femoral artery disease
- Popliteal artery disease
- Crural artery disease
Q4.5: What are the manifestations of common femoral disease?
Answer: Thigh and calf claudication.
Rapid Revision Reignite is designed to give you an edge in your final prep with Q&E Notes in a Question-Answer format, RR LIVE Classes for same-day explanations, and a refined QBank of 3,000 curated exam-style questions—making your preparation smarter, faster, and more effective.
Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Smarter Video Lectures also in हिंglish, Game Changing Qbank, Audio QBank, Structured Notes, Treasures, Mock test for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Facial Injuries And Abnormalities
Detailed Questions