Acromegaly- Clinical Features, Diagnosis, Treatment
Jan 9, 2024

It is a disorder related to the growth hormone (GH). Pituitary tumours are the common cause for increasing growth hormone.
Disorders of growth hormone depending on age- Increase in growth hormone in children before the fusion of bones - Gigantism.
Increase in growth hormone in adults after bone fusion - Acromegaly. Decrease in growth hormone before bone fusion - Dwarfism.
Growth hormone receptor resistance - Laron Dwarfism Growth hormone is synthesised in anterior pituitary. Growth hormone release hormone from hypothalamus is required.
Hypothalamus-GHRH, acts on somatotrophs of anterior pituitary. Release of GH from anterior pituitary. GH acts on liver (target organ). IGF-1/ somatomedin is released, acts on skeletal tissue/ soft tissue. Shows physiological actions of GH.
IGF-1 in excess quantity leads to activation of negative feedback mechanism. Further GH release do not occur. Increased IGF-1 inhibits GH secretion from anterior pituitary. IGF-1 stimulates hypothalamus, release of somatostatin , inhibits anterior pituitary. Further GH release don’t occur.
Aetiology
- Pituitary adenomas originate from somatotroph cells. Lactotrophs – Prolactin, Thyrotrophs – TSH, Corticotrophs – ACTH, Somatotrophs – GH, Gonadotrophs - FSH & LH
- 2 forms of pituitary adenomas. Macro adenoma: >1cm, more common, 75% cases. Mass effect on surrounding structures. Microadenoma: <1cm, only endocrine manifestations
- Rarely ectopic tumours also produce GH or GHRH causes Acromegaly . Mostly benign, <1% are malignant. GH is produced by 20% of pituitary tumours, Somatotrophs type. Mammosomatotroph pituitary adenomas produce excess prolactin + excess GH.
Clinical features
- Maximim GH secretion in 3rd to 5th decade of life . Clinical manifestations due to skeletal tissue overgrowth- Length of the bone do not increase, horizontal aspect increases, seen in face, skull, upper and lower limbs, joints.
| Face | Coarse facial features Frontal bossing Broad nose Prognathism Widely spaced teeth  |
| Skull | Head circumference increases Cap size increases |
| Upper limb | Swollen fingers Increase in ring size. Increase in glove size. Wrist joints are affected. 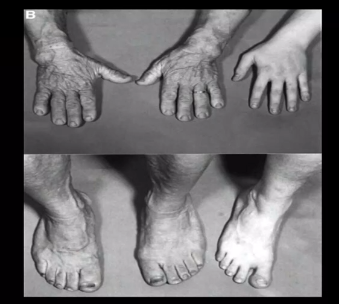 |
| Lower limb | Broad feet Increase in shoe size |
| Joints | Arthritis |
Also Read: Metabolic Syndrome- NEET SS Medicine
Clinical manifestations due to soft tissue overgrowth
|
Skin |
|
|
Tongue |
|
|
Internal organs |
|
|
Neurological manifestations |
|
|
Heart |
|
|
GIT |
|
|
CNS |
|
Mass effect of tumour, Impaired metabolism
|
Impairment of Carbohydrate metabolism |
|
|
Impairment of Lipid metabolism |
|
- Mammosomatotroph: Increased prolactin and GH. In females, menstrual irregularities (Amenorrhea, Galactorrhoea and Infertility (decreased ovulation). In males, decreased libido, spermatogenesis is affected. Infertility.
Diagnosis
- Best initial test: IGF-1 levels. Screening of somatomedins, normal: 90-370 ng/ml. Significant increase- positive screening test. Must be elevated 5 times the basal value. More IGF1, more is the severity. Random GH assay should not be done. GH secretion is episodic and pulsatile, Occurs during the day. Single random GH levels- no use. Serum GH levels: <1 mcg/L. Excludes the diagnosis of acromegaly. Confirmatory test: GH suppression test-Failure of GH suppression in response to glucose load.
Basic physiology
- Decrease in blood glucose levels, activation of counter regulatory hormones. Stoppage of insulin secretion (compensatory mechanism). Increase in glucagon levels, steroids, GH, TSH, catecholamines. Increase the blood glucose levels. GH levels decreases or normal.
GH suppression test
- Glucose syrup is consumed (100g) orally: After 60 mins, estimate serum GH levels, estimated GH levels: <0.4mcg/L - Acromegaly is excluded. >0.4 mcg/L - Suggestive of acromegaly.
Radiological studies
- CT/ MRI: MRI> CT in localising the tumour. MRI shows tumour in 90% Acromegaly patients. X-Ray of the digits shows terminal phalanges - Tufting of fingers or toes, Isolated spade phalanx.

- Increased thickness of heel pad >21mm. Also seen in myxoedema, phenytoin toxicity, presence of callus, obesity, peripheral edema. Normal thickness: 13-21mm.
Also Read: Management of Inflammatory Bowel Disease (Ulcerative Colitis and Crohn's Disease)
Treatment
- Best treatment: Surgical resection. Transsphenoidal surgery rapid response. In 10-20% patients, hypopituitarism develops. GH levels returns to normal within 1hr. For the normalisation of IGF1, it takes 3-4 days.
Medical management
- Best drug: Somatostatin analogues or somatostatin receptor ligands. Exert therapeutic effect through SST2 receptor. Provided therapeutic effect through SST5 receptor. Expressed on GH producing tumours. These analogues are resistant to plasma degradation. Drugs - Octreotide and Lanreotide (long acting, injectable depot). These drugs reduce the GH levels. In 70% patients, tumour regression occurs.
|
Octreotide |
|
|
Lanreotide |
|
- Pasireotide: Long acting, Multi receptor ligand, binds to SST5. Efficacy is very high. Adverse effects -Higher prevalence of glucose intolerance. New onset DM. Adverse effects: Short lived. Suppress GI motility and secretions. Suffer with fat malabsorption and abdominal discomfort. Increased flatulence. Within 2 weeks, remission of ADRs is seen. Gallbladder contractility, gallbladder emptying is also reduced. In 30% patients, cholesterol gallstones are formed(asymptomatic).
- Other ADRs-Mild glucose intolerance: transient insulin separation. Asymptomatic bradycardia. Hypothyroxinaemia. Local reactions at the injection site. Other alternative agents: Dopamine agonists- Cabergoline, Bromocriptine.
- If surgery is not curative, dopamine agonists are given: In Persistent acromegaly – Raloxifene. selective oestrogen receptor modulator. Useful in both men & post-menopausal women, breast cancer women. Dose: 60mg BD. It normalises the IGF1 levels.
- Pegvisomant: a GH analogue, Antagonise endogenic GH. Blocks GH receptor in the liver. 2nd line agent. Other therapies: Radiotherapy- Works when surgery and drugs do not work. Cause slow resolution of the disease. 20% chances of development of hypopituitarism. Tumour size gets reduced. Combined treatment-Monthly SSA+ weekly/ biweekly Pegvisomant. Helpful in resistant patients.

Complications
- Local tumour effects: Raised intracranial pressure, headache, vomiting, seizures, coma and death. Compression on surrounding structures- Optic chiasma causing visual abnormality. Other complications- Congestive cardiac failure (most common cause of death). DM, Cord compression.
Also Read: Special Considerations in Diabetes Mellitus
Hope you found this blog helpful for your NEET SS Endocrinology Preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Aetiology
Clinical features
Clinical manifestations due to soft tissue overgrowth
Mass effect of tumour, Impaired metabolism
Diagnosis
Basic physiology
GH suppression test
Radiological studies
Treatment
Medical management
Complications
Top searching words
The most popular search terms used by aspirants
- NEET SS Medicine Endocrinology
- NEET SS Medicine Preparation