Renovascular Hypertension- Causes, Investigations and Management
Oct 26, 2023

Introduction
Most common cause of secondary and potentially curable hypertension. Renovascular hypertension- Constitutes to only 5% of all hypertensive cases. Renovascular hypertension is the cause of renal failure in 5-15% of those older than 50 years of age. Accounts for as many as 10-20% of the ESRD population.
Causes Of Renovascular Hypertension
The two main causes include: Atherosclerosis- constitutes to 60-80% of the cases and fibromuscular dysplasia. Other causes: Arterial aneurysm, arteriovenous malformation, extrinsic renal artery compression, Neurofibromatosis-1 and Williams syndrome.
When Do You Suspect Renovascular Hypertension?
Refractory hypertension with grade 3 and 4 along with hypertensive retinopathy. Refractory hypertension - BP remaining high even after treatment with multiple anti-hypertensive medications. Abrupt onset of moderate to severe hypertension. If onset of hypertension in <20 and >50 years of age. If there is unexplained worsening of renal function with or without hypertension or in association with use of ACE inhibitors or ARBs. If there is paradoxical worsening of hypertension with the use of diuretics. Unexplained recurrent episodes of heart failure: Flash pulmonary edema. Systolic-diastolic abdominal bruit that radiates to both flanks. Diffuse vascular disease and/or evidence of cholesterol embolization.
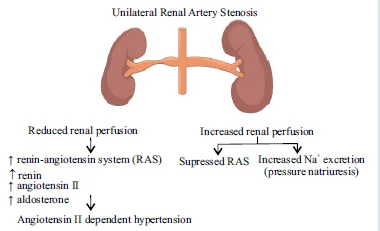
Two Kidney, One Clip Model (vasoconstrictor Hypertensive Model)
- It replicates human renovascular hypertension. In case, one of the renal arteries has undergone stenosis out of the two, the affected kidney will receive less blood flow. Due to this renin secretion is increased from the juxtaglomerular apparatus of the ischemic kidney and suppressed in the normal contralateral kidney. Due to this there is an increase in the volume leading to hypertension. The normal kidney removes the excess volume retained because of the renin. This model is also referred to as the Renin dependent model.
- Treatment: Unclipping of the “clipped kidney”/ACE inhibitors/ ARBs.
Also Read: Congenital Anomalies of the Kidneys and Urinary Tract
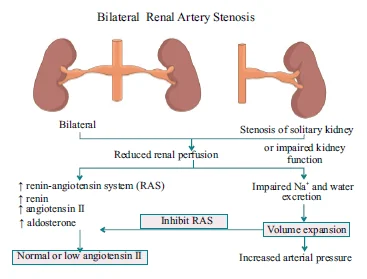
One Kidney, One Clip Model (Volume Hypertensive Model)
In an individual who possesses a single functional Kidney develops renal artery stenosis of that kidney or in a normal individual who develops B/L renal artery stenosis. Absence of a normal contralateral kidney prevents natriuresis and diuresis, leading to reduced blood flow to the kidney. Causes- intravascular volume expansion and renin secretion is suppressed in the clipped kidney because of feedback inhibition. This model is also referred to as volume dependent model.
Renovascular Hypertension Pathology
Decreased renal blood flow in renovascular hypertension leads to scarring, fibrosis and tubular damage. Less than 10% of the usual oxygen delivery is enough for normal renal tissue metabolism. If occlusion occurs >70-80% we call it critical stenosis. Histopathological changes: Biopsy reveals vascular stenosis, cholesterol crystals, tubular atrophy, interstitial fibrosis with inflammatory cells, a tubular glomeruli and focal or global glomerulosclerosis.
Renal Fibrosis Phases Of Eddy
The cellular activation and injury phase. The fibrogenic signalling phase. The fibrogenic phase and the destructive phase.
Also Read: Thyroid Gland - Anatomy, Embryology, Developmental abnormalities, Symptoms, Investigation

Renovascular Hypertension Diagnosis
- Duplex Ultrasound: Bed-side, Non-invasive investigation, helps calculate Resistive index. Resistive index= [1 - (end-diastolic velocity ÷ peak systolic velocity)] x 100. Higher RI (>1) suggests the presence of Renovascular hypertension. Can help predict improvement in BP and/or renal function following revascularization.
- CT Angiography (CTA): High sensitivity (98%) and specificity (94%). Not recommended if serum creatinine value is >1.7 due to contrast induced nephropathy.
- MR Angiography: Provides both anatomical and functional information. Lesions involving the distal, intrarenal and accessory arteries will be missed. Contraindicated if glomerular filtration rate (GFR) is less than 30 (G4 stage) due to Gadolinium induced Nephrogenic systemic fibrosis.
- Angiography: Both conventional renal angiography and intra-arterial DSA remain the gold standard for diagnosing renovascular disease. Reserved for cases where clinical suspicion is high or when intervention is planned. Intra-arterial DSA allows less radiocontrast to be administered (25 ml to 50 ml vs 100 ml) than the conventional renal angiogram and provides better anatomical detail.
Renovascular Hypertension Cause
Atherosclerosis Fibrous dysplasia 60-80% 20-40% (Medial 30%, Peri medial 5%, Intimal 5%) Seen in 40-70 years Seen in 20-50 years 80% proximal artery involvement Mostly distal artery involvement (towards the hilum of the kidney)
- There are 4 types of Fibrous dysplasia: 1. Median Fibroplasia, 2. Peri medial Fibroplasia, 3. Intimal Fibroplasia, 4. Medial Hyperplasia
1. Median Fibroplasia
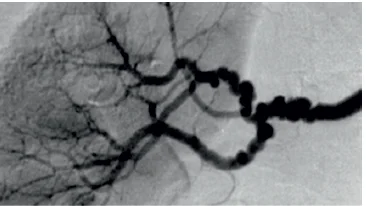
Exclusively in women between 25-50 years of age. “String of beads” appearance in angiography. Distal half of the main artery and branches involved. Not likely to progress to complete occlusion, nor are they likely to experience a decrease in their function.
2. Peri medial fibroplasia
- Exclusively in women between 5-15 years of age. Involves midrenal artery. “String of beads” appearance in angiography. Often progresses to renal occlusion and loss of renal function.
3. Intimal fibroplasia
- Approximately 10% of all cases, predominantly occur in children and young adults. Dissection, arterial wall hematoma and renal infarction occurs due to internal elastic lamina involvement. Usually, proximal renal artery is involved. Likely to progress and result in loss of renal function.
4. Medial Fibroplasia
- Angiographic findings indistinguishable from intimal hyperplasia. Histopathological examination reveals smooth muscle cell hyperplasia with no associated fibrosis. Renovascular hypertension is more likely to be observed when the lesion is ≥ 70% in one or both renal arteries or when a 50% stenosis with post stenotic dilatation is demonstrated. Clinical significance of a lesion may be determined by ACE inhibitors scans and by renal vein renin (RVR) measurements. Significant pressure gradient (>10-15 mmHg) across a renal artery lesion, which can be associated during intra-arterial renal angiography, may predict a reduction in BP with revascularization. An RVR ratio ≥ 1.5 (affected/non affected side) may be observed when the lesion is the cause of “renin-dependent” hypertension. RVR ratio is of poor predictive value in those with bilateral disease.
Also Read: RENAL STONES - Etiology, Investigation and Management
Renovascular Hypertension Treatment
- Medical Therapy: In about 90% of cases, effective control of blood pressure can be achieved through medical therapy alone. However atherosclerotic renal artery lesions may progress with time despite medical treatment. DOC- ACE inhibitors and ARBs.
- Angioplasty and Stenting: Indications for PTRA: Lesions >10 mm in length. Partially occluded and do not involve the ostium. Patients with a hemodynamically significant RAS. Accelerated hypertension or malignant hypertension. Hypertension with an unexplained unilateral small kidney. Hypertension with intolerance to medication
What is PTRA?
- Percutaneous transluminal renal artery angioplasty is an angiography technique by which stenotic renal arteries are dilated with a balloon-trippled catheter. Percutaneous transluminal renal artery with stenting- Atherosclerotic disease. Percutaneous transluminal renal artery without stenting- Fibromuscular dysplasia.
- Complications: Development of reversible acute renal failure thrombosis- Perforation, dissection of the renal arteries, diffuse atheroembolism. After successful percutaneous transluminal renal artery, an improvement in BP may be seen as quickly as 4-6 hrs after the procedure but is more commonly seen after 48 hrs, although the maximal anti-hypertensive effect may not be observed for several weeks. Restenosis rate following PTRA is significant (30% for Non Ostial and 50% for Ostial lesion). Therapeutic window- Serum creatinine level 1.5-3 mg/dl for interventions to be successful.
Recent studies
- These studies raise questions about the effectiveness of revascularization with stenting for BP control.
1. STAR trial
Enrolled 140 patients with BP controlled to <140/90 mmHg and with renal ostial >50%. Result- No difference in the degree of BP control between renal artery stenting and medical therapy or medical therapy alone.
2. ASTRAL trial
- Angioplasty and stenting for renal artery lesions. Enrolled 806 patients with atherosclerotic Ras to undergo renal artery stenting and medical therapy or medical therapy alone. Result- No difference in BP control, but anti-hypertensive medications required were slightly higher in the medically managed group.
3. CORAL trial
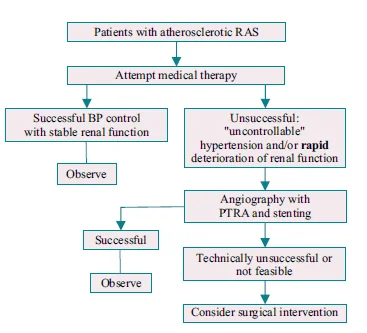
- Cardiovascular outcomes and Renal atherosclerotic lesions. Compared medical therapy alone with medical therapy + renal artery stenting in patients with atherosclerotic RAS and elevated BP, CKD, or both. Result- A reduction in systolic BP of a mean of 15-16 mmHg was achieved in both groups with an average of 3.4 medications, not different in either group. No long-term preservation of renal function was shown with vascular stenting in all the three studies. Treatment algorithm for patients with atherosclerotic RAS-
- Treatment algorithm for patients with fibromuscular dysplasia:

Also Read: Prune Belly Syndrome (Eagle Belly Syndrome)
Surgical Treatment Indications
- Concomitant aneurysmal or occlusive aortic disease. Macro aneurysms of the renal artery associated with stenosis. Malignant or accelerated HTN (with or without acute renal failure) who did not respond or cannot tolerate medical therapy. PTRA technically not feasible
Prerequisite for Surgical Treatment
- Kidney size >8 cm in length. Retrograde filling of the distal renal artery by collateral vessels on radiographic or scintigraphy imaging studies. Patency of the distal renal artery. Viability of the involved kidney on isotopic renography. Minimal glomerular sclerosis and well reserved tubules on renal biopsy.
Surgical Options
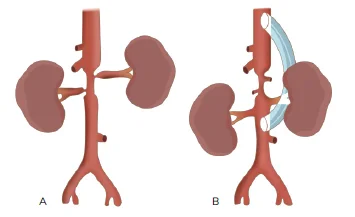
- Treatment of choice- Aortorenal bypass. Other options: Splenorenal bypass for left renal arterial lesions. Hepatorenal bypass for right arterial lesions. Ileorenal bypass, bench surgery with auto transplantation of the supraceliac or lower thoracic aorta for the bypass (if there is diffuse atherosclerotic disease).
Also Read: Post Operative Thyroid Complications
If you are preparing for NEET-SS 2024 and ahead, check out SS ELITE Plan (Version 4.0) and what makes it the perfect study resource for your super speciality preparation.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Causes Of Renovascular Hypertension
When Do You Suspect Renovascular Hypertension?
Two Kidney, One Clip Model (vasoconstrictor Hypertensive Model)
One Kidney, One Clip Model (Volume Hypertensive Model)
Renovascular Hypertension Pathology
Renal Fibrosis Phases Of Eddy
Renovascular Hypertension Diagnosis
Renovascular Hypertension Cause
1. Median Fibroplasia
2. Peri medial fibroplasia
3. Intimal fibroplasia
4. Medial Fibroplasia
Renovascular Hypertension Treatment
What is PTRA?
Recent studies
1. STAR trial
2. ASTRAL trial
3. CORAL trial
Surgical Treatment Indications
Prerequisite for Surgical Treatment
Surgical Options