Alternative Airway Devices and Adjuncts
Feb 13, 2023

Alternative Airway Devices and Adjuncts are important topics for the NEET PG exam because they play a critical role in the management of airway emergencies. Proper selection and use of alternative airway devices and adjuncts can make the difference between life and death for patients who are experiencing airway obstruction, respiratory distress, or cardiac arrest.
In order to effectively manage airway emergencies, healthcare providers must have a thorough understanding of the different types of alternative airway devices and adjuncts that are available, their indications for use, and the proper techniques for their insertion and maintenance.
This includes knowledge of various devices such as laryngeal mask airway (LMA), supraglottic airway devices (SGDs), and endotracheal tubes, as well as adjuncts such as oxygen masks, bag-valve-mask (BVM) devices, and chest compression devices.
In summary, the knowledge and skills related to Alternative Airway Devices and Adjuncts is essential for healthcare professionals, and is therefore an important topic in the NEET PG exam.
To ensure that your preparation for this important topic is complete, read this medical notes blog.

Overview
- If the equipment is above the glottis: Supraglottic.
- If the equipment is below the glottis: Infraglottic.
Important information
- Supraglottic
- Laryngeal mask airway
- Infraglottic
- Endotracheal tube
AIRWAY MANEUVERS TO OPEN AN OBSTRUCTED AIRWAY
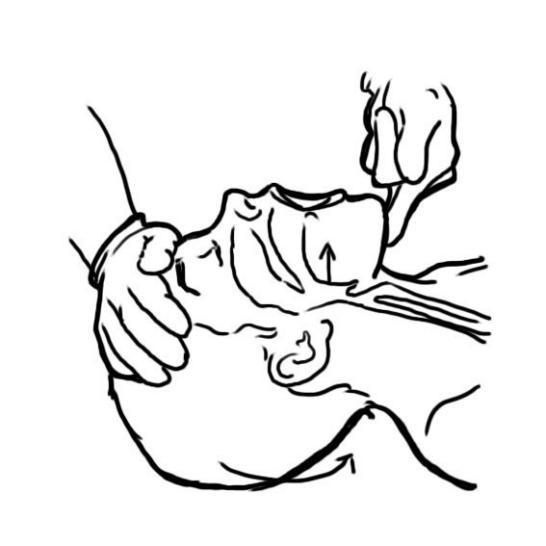
- Head tilt and chin lift
Pulls the tongue away from the airway and removes the obstruction.
- In trauma patients with suspected neck or cervical injuries, this maneuver is not performed.
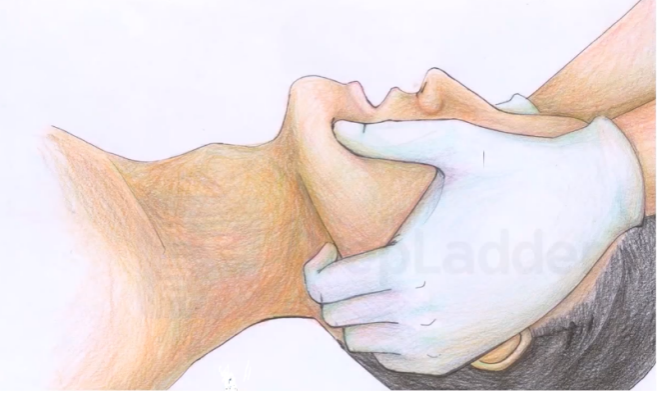
- Jaw lift or Jaw thrust
Forward protrusion of jaw. Head is in neutral position and forward protrusion of the jaw with head kept stabilized in both hands.
Important Information
- For trauma patients, since head tilt and chin lift maneuver involve neck movement.
- Therefore, we perform jaw lift maneuver in order to open airway.
Simple Airway Adjunct
Oropharyngeal Airway

Most common is Guedel’s airway. It is made up of rigid plastic. The size is determined from the angle of the lips to the angle of the mandible. It is inserted in an upside down position with a tip facing the roof of the mouth. Once it is half inserted, it is rotated to 180°.

Nasopharyngeal airway
In a conscious patient with compromised airway, we use nasopharyngeal airway. It is made up of soft silicon. The size is determined from the tip of the nose/ nostril to ear lobe. We insert it through the nasal cavity bevel facing the septum. It is a comfortable device. It can be inserted in a conscious patient.

ENDOTRACHEAL INTUBATION (ET)
- ET tube through oral cavity: Need Laryngoscope
- Popular used Laryngoscope is Mcintosh (Curved Blade Laryngoscope)

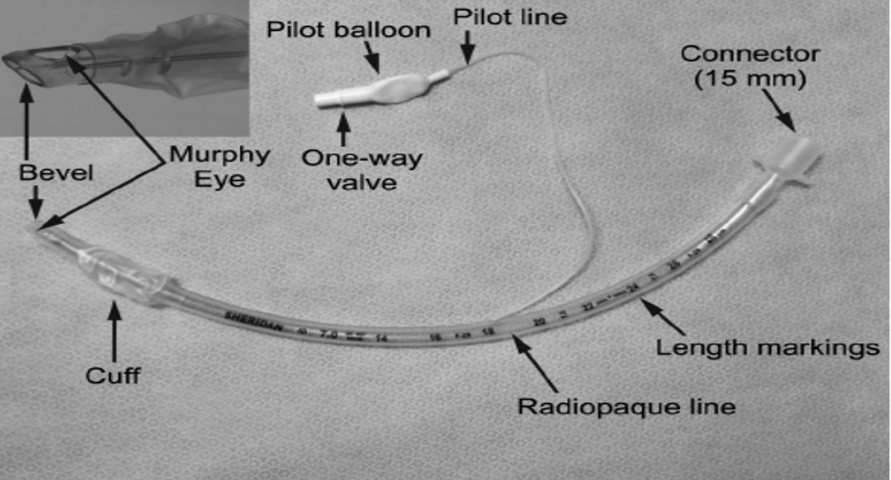
Parts of ET tube
- Glottic opening: Beveled to give a better visualization of glottic opening.
- Murphy’s eye: Alternate opening, if the terminal opening gets blocked or obstructed.
- Cuff: Creates a seal in trachea for positive pressure ventilation. It also prevents any upper secretions of the upper airway to go into lower airways, thus preventing the aspiration.
- Black mark: Left at the glottic opening, for the correct positioning of the tube. The ET tube is kept 3-4 cm above the carina.
- Universal connector: Connects to the circuit.

STEPS OF LARYNGOSCOPY AND INTUBATION
- Positioning: Morning sniffing position/ barking dog position
- Atlanto-occipital joint–extended.
- Neck-joint–flexed.
- Hold the laryngoscope in the left hand.
- Introduce the laryngoscope from the right angle of mouth. Sweep the tongue from the middle to the left side.
- Visualize epiglottis and Arytenoid/ Vallecula.
- Hinge the tip of the Laryngoscope in Vallecula and lift it.
- Inflate the cuff after introducing the tube.
- Check for the right position either through auscultation or capnography.
- Fix the tube.
SOME SPECIAL TUBES
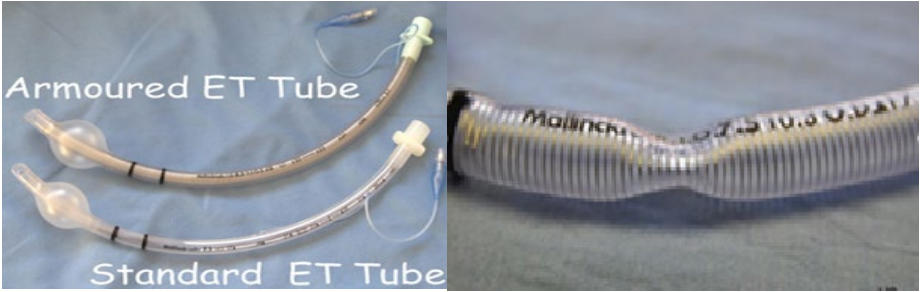
Flexometallic/ Armored tube/ Reinforced tube
- Inner diameter reinforced by metallic wire to make it kink resistant.
- Indications of using flexometallic tube
- Neuro surgery
- Head and neck surgery
- Prone position surgery

Important Information
- Differences b/w Flexometallic tube and standard ET tube. In flexometallic tube
- Universal connector is fixed.
- Highly malleable (rigid) so always needs a stylet during insertion.
- No radio opaque line required.
- It is kink resistant.
Double lumen tube
- It has 2 lumens
- Bronchus lumen: Going into either bronchus.
- Tracheal lumen: Going into trachea.
- It is used for one lung ventilation.
- Indications: Lung separation & Thoracic surgery.

RAE tube
- Ring - Aladdin – Elwyn tube.
- Specially designed for cleft-lip palate surgery.
- Bent in one direction either upward or lower direction.
- Not popular these days.
Uncuffed tube
- Used in pediatric < 7-9 years to prevent subglottic edema/ injury.
- Miller/straight blade laryngoscope is used in pediatric cases.
Important Information
- Indications of intubation
- During general anesthesia
- For positive pressure ventilation
- To protect the airway from aspiration
- For pulmonary toileting
ALTERNATIVE AIRWAY
Laryngeal Mask Airway (LMA): Supraglottic
- Classical LMA
- Designed by Dr Archie Brain
- Supraglottic airway device
- Easy and fast to insert
- Less invasive
- Not a definitive device
- Tip of classical LMA goes into hypopharynx (not glottic opening)
- Aspiration cannot be prevented
Important Information
- ET tube is the best device to prevent aspiration, cuff pressure necessary is 20-25 cm H2O/ 18-20 mmHg

- In this image the tip of cuff goes to hypopharynx and rest on hypopharynx
- The opening on ventral side will fall on the glottic opening
Pro seal LMA

- Has inflatable cuff
- Gastric tube
- Airway tube
|
First generation |
Second generation |
|
|
|
|
|
Sizes of LMA (Classic and Proseal) |
|
|
Weight in Kg |
Size of LMA |
|
< 5 kg 5-10 kg 10-20 kg 20-30 kg 30-50 kg 50-70 kg > 70 kg > 100 kg |
1 1.5 2 2.5 3 4 5 6 |

- I-gel: Non inflatable has a special polymer, this swells in the oral cavity and seals over the glottic cavity.
- It has airway and gastric tube through which can pass Ryle’s tube
- LMA supreme: Tube is curved so that it facilitates in the oral cavity.
Important Information
- Cervical spine injury
- In emergency: Manual in-line stabilization (MILS) of head and Oro-tracheal intubation.
- Elective: Fiber optic nasal intubation.
- Maxillo facial injury
- Emergency: Orotracheal intubation
- Elective: Tracheostomy
Also Read: Papulosquamous Disorders : Types and Treatment - NEET PG Dermatology
Previous Year Questions
Q. Steps of intubation, Arrange in sequence? (AIIMS Nov 2019)
A. Head extension and flexion of neck
B. Introduction of laryngoscope
C. Inflation of cuff
D. Check breath sounds with stethoscope
Ans: A-B-C-D
Q. Identify the device? (FMGE Aug 2020)

A. Endotracheal tube
B. Double lumen endotracheal tube
C. Laryngeal Mask Airway
D. Flexometallic tube
Q. Identify the following device? (FMGE Aug 2020)

A. Classical laryngeal mask airway
B. Proseal LMA
C. I-gel
D. LMA supreme
Q. Airway resistance to flow of gases through the endotracheal tube is due to?
(FMGE June 2021)
A. Diameter
B. Curvature
C. Length
D. Material
Q. Measurement of nasogastric tube? (INI-CET Nov 2021)
A. From angle of mouth to the below the ear lobe till xiphisternum
B. From tip of nose to below the ear lobe till manubrium sterni
C. From tip of nose to ear lobule to midpoint between manubrium sternii and umbilicus
D. From tip of the nose to below the ear lobe till umbilicus
We hope this blog was helpful and will aid your NEET PG exam preparations. You can also download the PrepLadder app and get access to relevant study content, video lectures and much more.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Overview
AIRWAY MANEUVERS TO OPEN AN OBSTRUCTED AIRWAY
Simple Airway Adjunct
Oropharyngeal Airway
Nasopharyngeal airway
ENDOTRACHEAL INTUBATION (ET)
Parts of ET tube
STEPS OF LARYNGOSCOPY AND INTUBATION
SOME SPECIAL TUBES
Flexometallic/ Armored tube/ Reinforced tube