Rapid Revision Reignite ENT: Question–Answer Format
Sep 17, 2025
Inner Ear Diseases And Facial Nerve
Detailed Questions
Q1.1: What is the benign tumor of the middle ear that arises from paraganglionic cells, and what is its site of origin?
Answer:
- Glomus tumour - Benign, locally invasive, slow growing tumour
- Glomus tumor originates from paraganglionic cells
- Cells of sympathetic nervous system which secrete catecholamines - epinephrine, norepinephrine, dopamine
- Usually present across major blood vessels like internal carotid artery, internal jugular vein
- In the middle ear, floor is related to the internal jugular vein and on the promontory (formed by the basal turn of ganglia), a plexus is formed - tympanic plexus - formed by glossopharyngeal nerve and sympathetic plexus of Carotid
- From these sympathetic plexus and the sympathetic plexus covering the internal jugular vein the tumor arises.
Q1.2: What is the difference between Glomus jugulare and Glomus tympanicum?
Answer:
- Glomus jugulare: Arising from the sympathetic plexus covering the internal jugular vein
- Glomus tympanicum: Arising from the tympanic plexus
Q.1.3: What is the pattern all paragangliomas have on HPE?
Answer: Typically, all paragangliomas have a pattern on HPE, known as Zellballen pattern.
Q.1.4: What are the symptoms of glomus tumor?
Answer:
- Sweating, flushing, headache, tachycardia (due to excess catecholamines)
- Conductive hearing loss - gradually progressive type(due to the mass growing)
- Pulsatile tinnitus (resembles the heartbeat)
- Pain + bleeding (as tumor lacks tunica media/ smooth muscle layer). Hence, probe test, biopsy, FNAC shouldn't be done th th th o
- If it involves the jugular foramen, it can cause 9 , 10 , 11 nerve palsies
- It can also cause Horner's syndrome
Q.1.5: Describe the signs of Glomus tumor.
Answer: Signs:
- Reddish hue from the floor of the middle ear: Rising sun appearance
- Seen on otoscopy
- Browns sign: When the pressure on the EAC is increased, tumor vibrates vigorously and then becomes pale
- Salt and pepper appearance - seen on a contrast enhanced MRI
- Phelps sign - seen on a CT scan: Tumor eroding the bone between the carotid artery and jugular vein
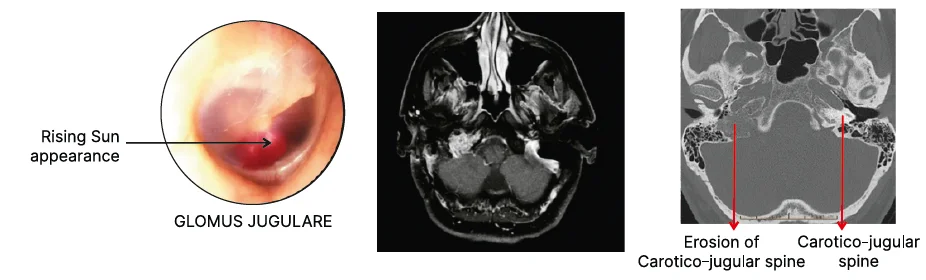
Q1.6: What is the IOC for glomus tumors?
Answer: IOC: CECT
- MRI can be done to check for intracranial spread
- Angiography to identify the feeding vessel
Q1.7: What is the treatment of glomus tumor? Name the classification of glomus tumor.
Answer:
- Treatment
- Angiography and embolize the feeding vessel
- Surgical excision
- Classification of glomus tumors: FISCH classification
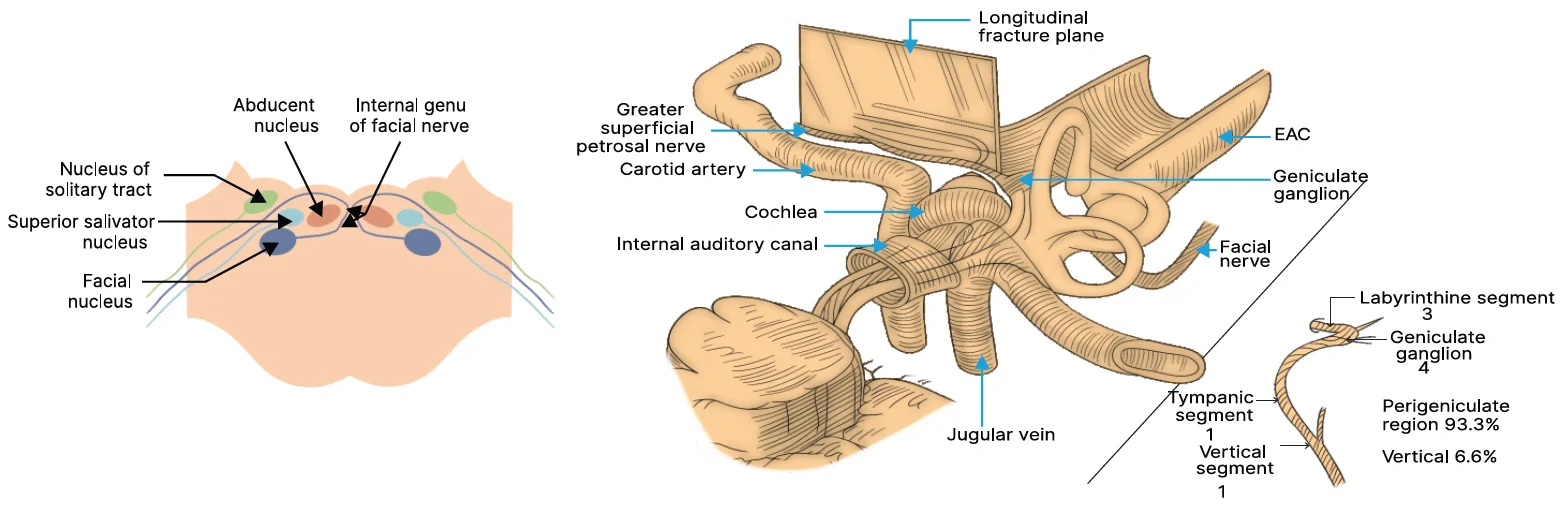
Q1.8: Describe the anatomy of the facial nerve.
Answer:
- 7TH cranial nerve that exits from pons
- Facial nerve nucleus is present in the brain stem
- Supranuclear palsy: Any lesion above the level of pons
- Infranuclear palsy: Any lesion below the level of pons
- Forehead is spared as it receives its innervation from bilateral cerebral cortex
- It is a mixed nerve having sensory root (nerve of Wrisberg), motor root and secretomotor root
- Course of facial nerve is divided into 3 parts:
- Intracranial
- Intratemporal
- Extracranial
Q.1.9: Describe the Intracranial route of facial nerve.
Answer: Facial nerve exits from its nucleus takes a turn around the nucleus of 6th nerve (facial colliculus) and emerges outside and enters the internal auditory canal.
Congenital Anomalies/Nasal Polyps/Rhinitis/Sinusitis
Big Question 2: Describe Meningocele, Glioma, and Dermoid swellings.
Broad Answer:
| Meningocele | Glioma | Dermoid | |
| Cause | Improper fusion of bones of base of skull or roof of nasal cavity | No fusion → herniation → delayed fusion | Hamartoma: A congenital anomaly |
| Consistency of swelling | Soft/ Cystic | Firm | Variable |
| Compressibility test | Positive | Negative | Positive |
| Reducibility test | Positive | Negative | Negative |
| Cough impulse test | Positive | Negative | Negative |
| Transillumination test | Positive | Negative | Negative |
| Treatment | Excision + Reconstruction | Excision | Excision |
Detailed Questions
Q2.1: What is Meningocele?
Answer: Herniation of meninges +/- brain tissue (meningoencephalocele) into the nasal cavity.
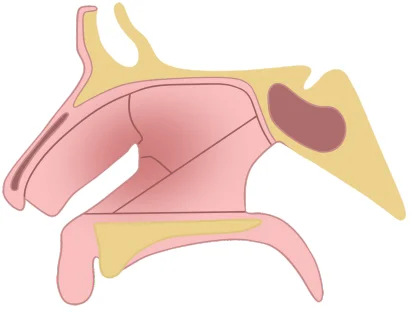
Q2.2: What are the bones forming the roof of the nose from anterior to posterior?
Answer: Frontal bone (Anteriorly), Cribriform plate (Middle), Sphenoid bone (Posteriorly).
Q2.3: Explain the cause of a Meningocele. What happens during development?
Answer:
- It is caused by improper fusion of bones of the base of the skull or roof of the nasal cavity.
- During development, if there is a deficient or dehiscent area in the bones, herniation of meninges (and sometimes brain tissue, meningoencephalocele) can occur through this gap into the nasal cavity.
Q2.4: Describe the consistency and the results of compressibility, reducibility, cough impulse, and transillumination tests for a Meningocele.
Answer:
- Consistency: Soft/Cystic
- Compressibility test: Positive
- Reducibility test: Positive
- Cough impulse test: Positive
- Transillumination test: Positive
Q2.5: What is the treatment for a Meningocele?
Answer: Excision of the herniated mass and reconstruction of the defect.
Q2.6: What is Glioma?
Answer: A condition in which there is presence of glial cells outside the central nervous system.
Q2.7: Explain the cause and formation of a Glioma in the nasal cavity.
Answer: Initially, there is improper fusion of bones in the roof of the nose, leading to herniation of cranial contents into the nose. Later, delayed fusion of bones separates the cranial cavity from the nasal cavity. During this process, CNS tissue (glial cells) gets left behind in the nasal cavity. Nasal immune cells then identify the glioma as foreign, causing an antigen-antibody reaction and subsequent fibrosis.
Big Question 3: Describe Septal Abscess and Septal Hematoma?
Broad Answer:

- Septal Abscess is a collection of pus caused by trauma/infection, presenting with bilateral nasal obstruction, headache, fever, and lymphadenopathy.
- Septal Hematoma is a collection of blood due to trauma, presenting with bilateral nasal obstruction and headache, but typically without fever or lymphadenopathy.
- Presentation for both septal abscess and septal hematoma is same
- Swelling on either side of septum
.jpg)
Detailed Questions
Q3.1: What are the typical causes of a Septal Abscess versus a Septal Hematoma?
Answer:
- Septal Abscess: Trauma, nasal infection, iatrogenic, nasal picking.
- Septal Hematoma: Trauma (direct, surgical, iatrogenic).
Q3.2: How do the clinical presentations of Septal Abscess and Septal Hematoma differ, particularly regarding headache, lymphadenopathy, and fever?
Answer:
| Septal abscess | Septal hematoma | |
| Presentation | H/O trauma +/- B/L nasal obstruction | H/O trauma +B/L nasal obstruction |
| Headache | + | +/- |
| Lymphadenopathy | + | - |
| Fever | + | - |
Q3.3: Why is early intervention more crucial for a Septal Abscess compared to a Septal Hematoma?
Answer: Early intervention is more crucial for a septal abscess because it is located in the danger triangle of the face (between the nasion and angle of the lips), meaning infection can spread to the cavernous sinus, leading to cavernous sinus thrombosis.
Q3.4: What is the treatment for a Septal Abscess, and what is the treatment for a Septal Hematoma?
Answer:
- Septal Abscess: Incision and drainage + Intravenous (I.V.) antibiotics.
- Septal Hematom: Incision and drainage + Pressure packing.
Q3.5: Compare Septal Abscess and Septal Hematoma regarding risk of complications and recurrence.
Answer:
- Septal Abscess: Higher risk of complication, higher risk of recurrence.
- Septal Hematoma: Lower risk of complication, lower risk of recurrence.
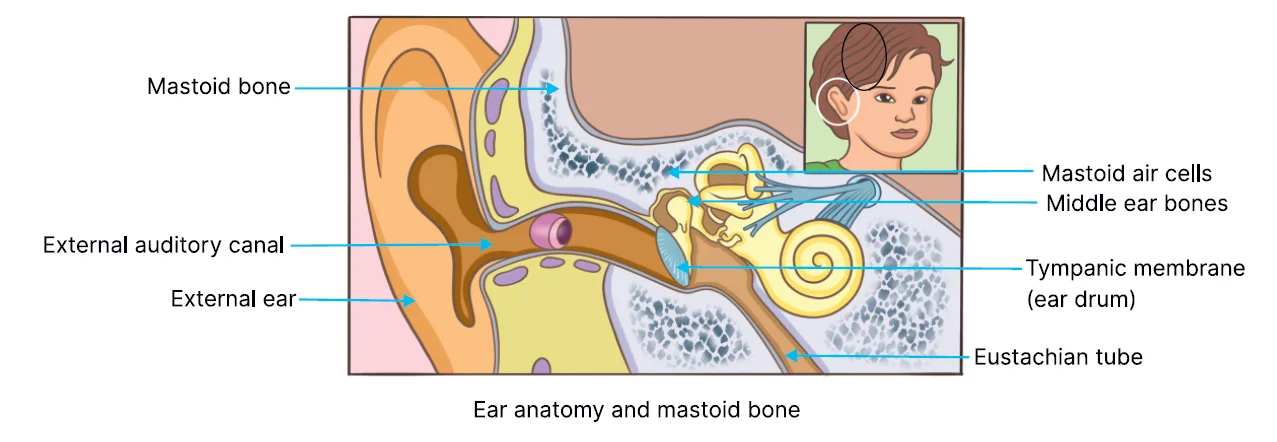
Anatomy of Ear
Big Question 4: What are the anatomical components and features of the human ear?
Broad Answer:
The human ear is anatomically divided into three main parts: the external ear, middle ear, and inner ear. Each part has specific structures that play roles in hearing and balance. The external ear includes the pinna, external auditory canal, and tympanic membrane. The middle ear involves air-filled cavities, ossicles, and the Eustachian tube, while the inner ear consists of the bony and membranous labyrinth involved in hearing and equilibrium.
Detailed Questions:
Q4.1: What are the three parts of the external ear?
Answer:
- Pinna
- External auditory canal (EAC)
- Tympanic membrane
Q4.2: What are the anatomical features of the pinna?
Answer:
- Made up of elastic cartilage
- Areas devoid of cartilage:
- Incisura terminalis (space between tragus and helix)
- Ear lobule
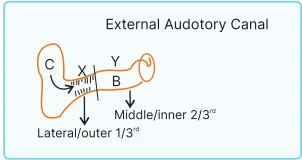
Q4.3: What is the external auditory canal (EAC) and what are its features?
Answer:
- Continuation of the pinna
- Length: 24 mm
- Two parts:
- Cartilaginous part (outer third) → 8 mm
- Bony part (inner two-thirds) → 16 mm
- Shape: S-shaped
- Contains hair follicles, sebaceous glands, and ceruminous glands (in the cartilaginous part only)
- Absent in bony part
- Infections like otitis externa/folliculitis (Staphylococcus) occur in cartilaginous part
Q4.4: What is the clinical relevance of the Incisura terminalis?
Answer:
- It is the site of incision in endaural surgery.
- The incision is called the Lempert endaural incision.
Q4.5: Differentiate between cartilaginous and bony parts of the external auditory canal?
| Cartilaginous part | Bony part |
| It is the lateral or outer part. | It is the medial or inner part. |
| It accounts for 1/3rd length of EAC i.e., 8mm. | It accounts for 2/3rd length of EAC i.e., 16mm |
| Hair follicles, sebaceous glands and ceruminous are present | Hair follicles, sebaceous glands and ceruminous are absent |
| Otitis externa or folliculitis (staphylococcus infection) are seen | Not seen |
Fractures of Facial Skeleton And Tumors of Nose And PNS
Big Question 5: How are the facial skeleton fractures classified?
Broad Answer:
- Facial skeleton fractures are classified into
- Upper
- Middle: nasal bone fractures are most common
- Lower
Detailed Questions
Q5.1: What are the types of nasal bone fractures?
Answer
| Class 1 | Chevallet fracture |
| Class 2 | Jarjaway fracture |
| Class 3 | Naso-orbito-ethmoid fracture |
Q5.2: Which type of fracture is most common in the middle third of the facial skeleton?
Answer:
- Fractures of the nose.
- A zygomatic fracture is the second most common fracture after the nasal bone fracture.
Q5.3: Describe the characteristic deformity and risk associated with Naso-orbito-ethmoid (NOE) fracture.
Answer: "Pig nose deformity," where the orbit and ethmoid bone are depressed, and the rest of the dorsum of the nose gets pushed in an upward direction. There is a high chance of CSF leakage because the fracture is very close to the cribriform plate of the ethmoid.
Q5.4: Differentiate between class 1 and class 2 fractures based on direction of blow and fracture.
Answer:
| Jarjaway fracture (Class 2) | Chevallet fracture (Class 1) | |
| Direction of blow | From front | From below |
| Direction of fracture | Horizontal | Vertical |
Jarjaway fracture (Class 2) - Direction of fracture - Horizontal
Chevallet fracture (Class 1) - Direction of fracture - Vertical
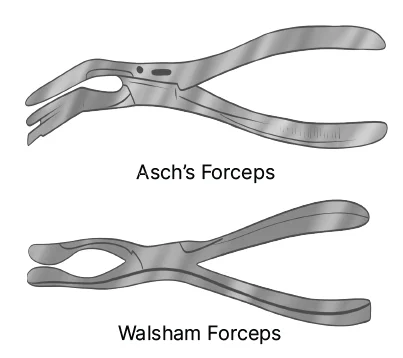
Q5.5: Name the two specific forceps for reducing nasal and septal fractures?
Answer:
- ASH Septum Forceps (for reducing septum fractures)
- Walsham Forceps (for reducing nasal bone fractures)
If you’re looking to strengthen your final prep, don’t miss out on Rapid Revision Reignite in Question-Answer format by PrepLadder. It’s designed to help Medical PG aspirants cover the entire syllabus quickly with concise notes in a Question-Answer format, high-yield MCQs, and expert-led revision videos—perfect for last-minute reinforcement before the exam.
Download the PrepLadder app now to access high-yield content with 24-hr Free Trial. Explore premium study resources like Video Lectures also in हिंglish, digital notes, Audio QBank, and Mock Tests for a seamless exam preparation. Get started with NEET PG coaching online with PrepLadder.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Inner Ear Diseases And Facial Nerve
Detailed Questions
Congenital Anomalies/Nasal Polyps/Rhinitis/Sinusitis
Detailed Questions
Detailed Questions
Anatomy of Ear
Detailed Questions:
Fractures of Facial Skeleton And Tumors of Nose And PNS
Detailed Questions
Top searching words
The most popular search terms used by aspirants
- NEET PG ENT
- NEET PG ENT Preparation
- NEET PG Preparation
- Rapid Revision
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial