Rapid Revision Reignite for Medicine: Question-Answer Format
Sep 5, 2025

Rheumatology
BIG QUESTION 1: Describe systemic sclerosis (scleroderma) with its key features, antibody profile, and complications.
Broad Answer:
- Systemic sclerosis is an autoimmune connective tissue disease marked by excessive collagen deposition, causing skin thickening, vasculopathy, and internal organ fibrosis.
- Diffuse type is associated with anti-Scl-70 and has widespread involvement; limited type presents as CREST syndrome with anti-centromere antibodies.
- The early sign is the Raynaud phenomenon (white→blue→red color change in digits).
- Skin changes include leather-like texture, salt-and-pepper pigmentation, and microstomia.
- Internal involvement includes esophageal dysmotility (↓LES tone), interstitial lung disease, and pulmonary artery hypertension (leading cause of death).
- Renal crisis with malignant hypertension is managed with ACE inhibitors.
Detailed Questions
Q1.1 Specify the antibodies of Scleroderma/Systemic Sclerosis
Answer:
- Anti-topoisomerase antibody present
- Anti-SCL-70 present
Q1.2 What are the clinical features of Scleroderma/Systemic sclerosis?
Answer:
- Fibrosis around blood vessels in the tips of the fingers, because of which the autoregulation of blood supply will be hampered
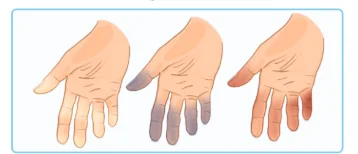
Q1.3 Explain the mechanism of the Raynaud phenomenon and its sequence of color change.
Answer:
- A lady in a cold environment, there could be a change in the color of the fingertips of this patient in the order:
Exaggerated vasoconstriction - White fingertips
↓
Due to vasoconstriction, there is less blood supply, and the concentration of deoxygenated Hb will rise - Cyanosis/ blue fingertips
↓
Exaggerated vasodilation
- Initially exaggerated vasoconstriction, then exaggerated vasodilation: Raynaud phenomenon
Q1.4 What are the early and characteristic skin changes in diffuse systemic sclerosis?
Answer:
- Early feature: Raynaud phenomenon
- Leather-like skin: Fibrosis under the skin
- Salt and pepper appearance of skin
Q1.5 Explain esophageal involvement in systemic sclerosis
Answer:
- Microstomia: Fibrosis can also occur in the mouth of these patients, so there may be difficulty in opening the mouth
- Oesophageal dysmotility: Fibrosis can occur in the esophagus, causing dysphagia
- In women, dysphagia is commonly seen with achalasia cardia
- To differentiate achalasia cardia from scleroderma, LES tone is checked
- Achalasia cardia: Loss of inhibitory control, so LES (Lower oesophageal sphincter) tone increases
- In scleroderma, Fibrosis in the LES, so the tone will be relatively less
- As a result, reflux oesophagitis can occur
Q1.6 Describe the major pulmonary complications of systemic sclerosis
Answer:
- Interstitial lung disease: Fibrosis in the lungs
- Pulmonary artery hypertension: Fibrosis in the pulmonary artery
- PAH: Loud P2
- DLCO (Diffusion in lung for carbon monoxide) values lesser: Fibrosis in the wall of the blood vessel
Q1.7 Describe the Scleroderma crisis and its management.
Answer:
- Scleroderma crisis: There will be a progressive decrease in the size of the kidneys
- GFR will be lower
- RAAS will be activated, causing hypertension
- Hypertensive crisis develops
- Management: ACE inhibitors (oral)
Q1.8 What is the leading cause of mortality in Scleroderma?
Answer:
- Leading cause of mortality in scleroderma: PAH
Q1.9 When is a heart–lung transplant preferred over a lung transplant in systemic sclerosis?
Answer:
- When severe PAH (>60 mmHg) is present
Q1.10 Describe the clinical features and management of CREST syndrome
Answer:
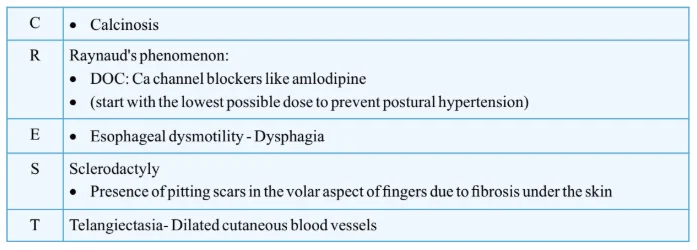
Q1.11 Which antibody is most commonly associated with CREST syndrome?
Answer:
- Anti-centromere antibody — highly specific
CARDIOLOGY
BIG QUESTION 2: How is infective endocarditis diagnosed, what are its major microbiological patterns, and when is prophylaxis indicated?
Broad Answer:
Infective endocarditis (IE) is diagnosed using the Modified Duke Criteria (major + minor criteria). Causative organisms vary depending on presentation (acute, subacute, IV drug user, prosthetic valve). Prophylaxis is indicated for certain high-risk cardiac lesions before dental procedures, but not for low-pressure shunts like ASD.
Detailed Questions
Q2.1: What are the Modified Duke Criteria for IE?
Answer:
- Major criteria:
- Positive blood culture with typical IE organisms (Viridans strep, Strep bovis, HACEK, Staph aureus, Enterococci without other focus) from ≥2 separate cultures; persistent positivity (2 drawn >12 h apart or majority of ≥4 with 1 h gap); or single positive for Coxiella burnetii / high IgG phase I titer (>1:800).
- Evidence of endocardial involvement:
- Echo: Vegetation, abscess, prosthetic valve dehiscence
- New valvular regurgitation (change in murmur alone not enough)
- Minor criteria:
- Predisposition (heart disease or IV drug use)
- Fever >38 °C
- Vascular phenomena (emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhage, Janeway lesions)
- Immunologic phenomena (GN, Osler nodes, Roth’s spots, rheumatoid factor)
- Positive blood culture not meeting major criteria
- Diagnosis:
- Definite IE: 2 major OR 1 major + 3 minor OR 5 minor
- Possible IE: 1 major + 1 minor OR 3 minor
Q2.2: What are the common causative organisms in different scenarios?
Answer:
- Acute bacterial IE: Staph aureus, Streptococcus (community-acquired)
- Subacute bacterial IE: Strep viridans
- IV drug abuser (right-sided IE): Staph aureus
- Prosthetic valve IE: Coagulase-negative Staphylococcus
Q2.3: How should blood cultures be taken in suspected IE?
Answer:
- At least 3–4 cultures, 1–2 h apart, before starting antibiotics
- Timing gap helps prove the heart is the bacterial source
- Coxiella burnetii (Q fever) may show only 1 positive culture out of 3
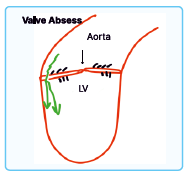
Q2.4: What are the echocardiographic findings in IE progression?
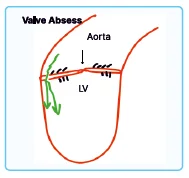
Answer:
- Vegetations → Valve Abscess → Leaflet Perforation → Regurgitation → New Murmur
Q2.5: When is antibiotic prophylaxis indicated for dental procedures?
Answer:
- Indicated in:
- Prosthetic heart valve
- LV assist device
- Prior endocarditis
- Certain congenital heart diseases (unrepaired, repaired <6 months, or repaired with residual defects)
- Transcatheter pulmonic valve
- Valvulopathy after cardiac transplantation
- Not indicated in:
- Low-pressure shunts like ASD (LA–RA gradient ~4 mmHg)
- Example: Ampicillin 1 h before procedure in indicated cases
- Low-pressure shunts like ASD (LA–RA gradient ~4 mmHg)
Q2.6: A 25-year-old patient with dental caries is undergoing dental extraction. Which of the following does not need prophylaxis for endocarditis?
A. Previous h/o endocarditis
B. Artificial heart valve
C. Untreated cyanotic heart disease
D. ASD
Answer: D
- ASD: Low-pressure shunt
- It operates at a pressure difference of only 4mmHg, LA-RA = 4mm Hg
- So antibiotic prophylaxis would not be required

Neurology
BIG QUESTION 3: What is the approach to thrombolysis in the acute management of ischemic stroke?
Broad Answer:
Thrombolysis in acute ischemic stroke is performed to restore cerebral blood flow within a specific time window, aiming to salvage brain tissue. Beyond this window, mechanical thrombectomy is considered up to 24 hours. Management includes airway stabilization, BP control, NIHSS-based severity assessment, antiplatelet and anticoagulant therapy, statins, and consideration of carotid endarterectomy if indicated.
Detailed Questions
Q3.1: What are the key radiological findings in acute ischemic stroke before thrombolysis?
Answer:
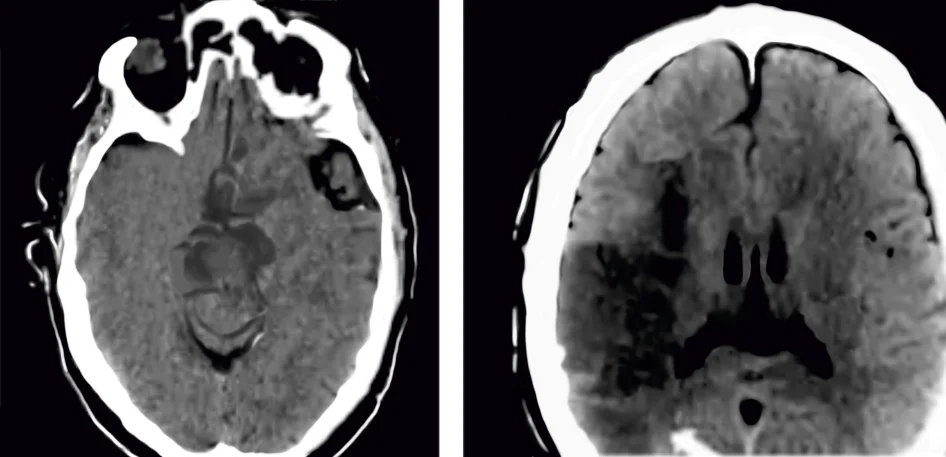
- Non-contrast CT head
- Normal in the majority
- Done initially to rule out haemorrhagic stroke
- One of the side effects seen with thrombolysis is an increase in the incidence of bleeding.
- Hyperdense MCA sign: Early finding; not seen in most cases.
- Hypodensity: Develops later with ischemic damage.
Q3.2: What is the recommended time window for thrombolysis in ischemic stroke?
Answer:
- General recommendation: Up to 4.5 hours
- USA: Up to 3 hours
- Canada & UK: Up to 4.5 hours
- Harrison’s latest edition: Benefit possible up to 6 hours
- So, thrombolysis can be done up to: 4.5-6 hours
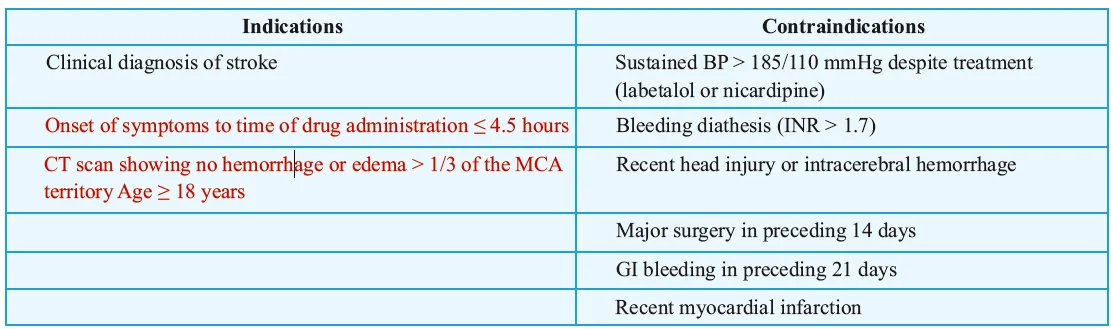
Q3.3: What are the indications and contraindications for thrombolysis?
Answer:
Q3.4: What are the drugs used in thrombolysis and their administration method?
Answer:
- Alteplase: Bolus followed by infusion
- Tenecteplase: Single bolus, can be given inside a CT scan after ruling out hemorrhage
Q3.5: What is the management pathway for acute ischemic stroke?
Answer:
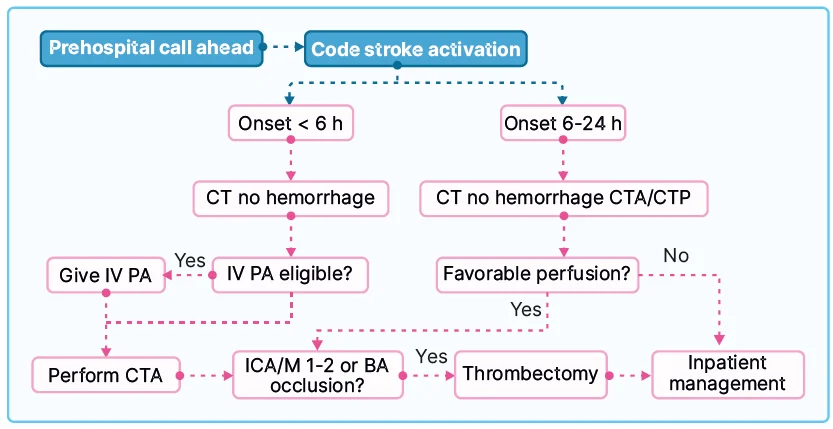
Q3.6: Which patients are eligible candidates for thrombolysis within the first 6 hours?
Answer:
- Age > 18 years
- No evidence of hemorrhage with respect to CT head
- Onset of symptoms (earlier detected/intervened, more brain tissue can be saved).
Q3.7: In which clinical scenario is Tenecteplase given to a stroke patient?
- When the patient has clinical features suggestive of stroke
- The CT scan is normal
- Evidence of hemorrhage is ruled out
Q3.8: What are the steps in the management of acute ischemic stroke?
Answer:
- Assess airway
- BP control
- Time last seen normally
- Evaluate the severity of stroke by NIHSS (National Institute of Health Stroke Severity)
- If NIHSS > 5
- Thrombolysis
- Endovascular therapy: MERCI
- Once an acute ischemic stroke is handled
- Then aspirin can be given after the first 24 hours, as it will prevent the redevelopment of stroke and reduce current mortality
- Ticagrelor: Loading dose 180 mg and subsequently 90 mg twice a day
- After 1 month: Ticagrelor will be discontinued and aspirin will be continued at a low dose for the whole life of this patient, 75- 81 mg, whichever is available (In Harrison: 81 mg)
- D.A.P.T.: Aspirin + Ticagrelor should be continued for 1 month, as it reduces the chances of reinfarction in these patients
- Statins
- Anticoagulant agents: Apixaban - Atrial fibrillation
- If it is rheumatic heart disease or mitral stenosis, then warfarin is given
- If there is atherosclerotic narrowing of the internal carotid artery, then either in the same hospitalization or maybe on a later admission, carotid endarterectomy can be done
- Achieve target systolic blood pressure
- Initially, SBP can be 130/140 to ensure cerebral perfusion
- Cerebral perfusion = Mean arterial pressure – Intracranial pressure
- But trials have shown that if a person has suffered from a stroke & once he is on the road to recovery/ handled the acute phase, then subsequently the target of BP in the range of 120 or less should be achieved.
Nephrology
BIG QUESTION 1: What are the different types of Dyselectrolytemias?
Broad answer: Dyselectrolytemias are imbalances of sodium, potassium, and magnesium. Hyponatremia can be hypovolemic or euvolemic, treated with fluids or restriction. Hypernatremia, often from dehydration, needs slow correction with hypotonic fluids. Hypokalemia causes ECG changes like ST depression and U waves, treated with potassium. Hyperkalemia and magnesium imbalances require urgent correction to prevent cardiac complications.
Detailed Questions:
Q.1.1: What is the formula for calculating total sodium deficit?
Answer:
- Female: Weight × 0.5 × [Desired value - Actual value]
- Male: Weight × 0.6 × [Desirable value - Actual value]
Q1.2: What are the key features of Hypovolemic Hyponatremia?
Answer:
- TBS: Decreased
- TBW: Decreased
- Causes:
- Diarrhea
- Vomiting
- Cerebral salt wasting syndrome
- Addison's Disease
- Treatment: · ORS and IVF
Q1.3: What are the key features of Euvolemic Hyponatremia?
Answer:
- TBW: Increased
- TBS: Normal
- Causes:
- SIADH: Causes of SIADH include Cerebral toxoplasmosis and Oat cell lung cancer
- Postoperative: Non-judicious use of IVF (overcorrection of IVF)
- Endurance sports
- Hypothyroidism: Thyroid hormones play an indirect role in the regulation of antidiuretic hormone
- Treatment: Fluid restriction and Vaptans (V2 receptor blocker)
Q1.4: What are the key features of Hypervolemic Hyponatremia?
Answer:
- TBW: Increased (water >> salt)
- TBS: Increased
- Causes:
- CHF
- Cirrhosis
- Chronic Kidney Disease
- Treatment: · Diuretics
Q1.5: What are the key features of Hyponatremia?
Answer:
- Dangerous Hyponatremia: Any value < 125 meq/L
- Fast correction of Hyponatremia will lead to Osmotic demyelination syndrome
- Manifestations that can occur in this patient: Stroke-like features
- Fluid of choice for correction of severe hyponatremia: 3% saline/ Hypertonic saline
- Value of Na+ in 3% saline = 514 meq/L
- Value of Na+ in 0.9 % saline = 154 meq/L
Q1.6: What are the key features and causes of Hypernatremia?
Answer:
- When the Na+ value is > 158meq, it is called dangerous hypernatremia (causes a shift of fluids across the brain, leading to seizures)
- Leading cause of Hypernatremia: Debility in old age (low water intake)
- Causes for the development of Hypernatremia (Mnemonic: MODEL)
- Medication - Lithium can contribute to nephrogenic diabetes insipidus, which causes loss of water from the body, and if this loss is not compensated, it will lead to Hypernatremia
- Osmotic diuresis
- Diabetic Insipidus (Central diabetic insipidus and Nephrogenic diabetic insipidus)
- Excessive H2O loss
- Low H2O intake
- Note: An Important cause of Hypernatremia in pediatrics is due to improperly diluted ORS, which causes doughy skin on examination
Q1.7: What are the clinical features and management of Hypernatremia?
Answer:
- Clinical features (Mnemonic: ) SALT
- Skin: Flushed
- Agitation
- Low-grade fever
- Increased thirst
- Investigation: Urine osmolarity
- <250 mosm: Diabetic insipidus
- > 400 mosm: Lactulose osmotic diarrhea
- Formula for correction in a symptomatic patient: TBW x (Actual Na - 140)/140
- Correction fluid: 5% Dextrose
- Asymptomatic Hypernatremia: Liberal intake of H2O
Q1.8: What are the key features of Hypokalemia?
Answer:
- Clinical features:
- Cramps
- Ileus
- Flaccid paralysis: if weakness persists in spite of potassium correction, then the electrolyte imbalance is Hypomagnesemia
- Cause of death: Diaphragmatic paralysis
- CVS arrhythmia: Torsades De pointes → Both hypokalemia and hypomagnesemia can trigger torsades de pointes
- Trans tubular potassium gradient- if value is > 4, it indicates renal wasting → Two important causes of renal wasting are Gitelman syndrome (problem will be in DCT) and Bartter syndrome (Problem in thick ascending loop of Henle)
Q1.9: What is Pseudo-P-Pulmonale?
Answer:
- P-pulmonale is a p-wave more than 2.5mm in the presence of pulmonary artery HTN. Here, there is no Pulmonary artery HTN, so we call it pseudo-P-Pulmonale
- Whenever potassium goes down, ST ↓, T-wave inversion, QU interval prolongation, and a Prominent U wave occur.
Q1.10: What is the Correction rule for Hyokalemia?
Answer:
- For value 3.0- 3.5 meq/L: ORAL
- For value <3.0 meq/L: IV
- 1ml KCl=2meq
- 1ampoule=10ml KCl contains 20 meq
- 20 meq causes potassium in the blood to rise by 0.25 meq
Q1.11: What are the ECG Findings of Hyperkalemia?
Answer:
- Tall, tented T-waves
- ST elevation
Q1.12: What is the Treatment of Hyperkalemia?
Answer:
- Mnemonic: CABG-D2
- Calcium gluconate: Antagonizes the action of potassium on the heart
- Albuterol nebulization
- Bicarbonate: It is not used routinely; used when a patient is having metabolic acidosis concomitantly
- Glucose + Insulin: The objective of giving insulin to the patient is to send potassium inside the cell. Insulin drip is one of the most effective drugs to treat dangerous hyperkalemia. The magnitude of fall is 0.5-1 meq /hr
- Diuretic: Loop diuretics cause, i.e., urinary loss of potassium, Kaliuria
- Most effective method: Dialysis
- For chronic Hyperkalemia
- Patiromer + Sodium Polystyrene sulfonate (K+ Bind)
Q1.13: What are the causes of Hypomagnesemia?
Answer:
- Hypomagnesemia will be present in Chronic diarrhea, Alcoholics, Use of Thiazides (because of action on DCT), and Gitelman Syndrome
- TRPM6 is a receptor that helps in the reabsorption of Mg. Thiazides will block this receptor and congenital defect in Gitelman syndrome
- TRPM6 will not be working as a result, both thiazides and Gitelman syndrome cause magnesium wasting
- Magnesium antagonizes the effect of intracellular calcium.
Q1.14: What are the side effects of Hypomagnesemia?
Answer:
- Muscle cramps
- HTN: As Mg antagonizes the action of intracellular calcium, low magnesium levels will lead to increased calcium activity, i.e., Vasoconstrictio,n and cause HTN
- Increase in HR
- Risk of development of Torsades-de-pointes: Hypokalemia, hypomagnesemia, and Hypocalcemia can cause TDP
- Increased neuromuscular excitability can cause tremors, Nystagmus, and Athetosis
Q1.15: What is the Treatment of Hypomagnesemia?
Answer:
- Magnesium sulfate (depending on the deficit, it can be given parenterally/IM/IV)
- Oral: Magnesium oxide
Q1.16: What are the key features of Hypermagnesemia?
Answer:
- Normal values: 1.3-2.1 meq/L
- Death: If value goes > 10 meq/L, it can cause Asystole
- Causes:
- CKD
- Eclampsia: MgSO4 overdose
- Antacid, Laxative abuse
- Clinical features:
- Shock, which is not responding to IV fluids, vasopressor (earliest feature)
- DTR will decrease
- Urine output will decrease
- Respiratory rate will decrease
Q1.17: What is the treatment of Hypermagnesemia?
Answer:
- Vigorous Hydration
- DOC: Calcium gluconate
- Calcium gluconate is used in the treatment of Tetany, acute hyperkalemia, and acute hypermagnesemia.
- Hemodialysis
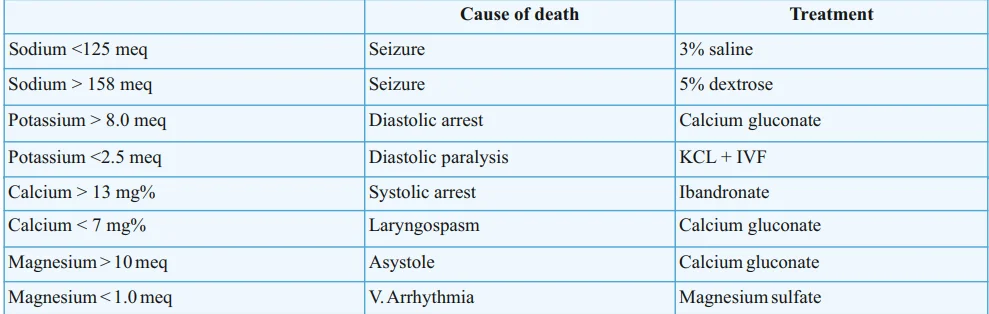
Q1.18: What are the causes of death and Treatment in different Dyselectrolytemias?
Answer:
Endocrinology
BIG QUESTION 1: What is Acromegaly and how is it diagnosed and managed?
Broad Answer:
Acromegaly is a hormonal disorder caused by excessive growth hormone secretion, usually due to a pituitary adenoma. Since it develops after puberty, patients do not become taller but instead show enlargement of extremities and characteristic facial changes. Diagnosis relies on biochemical tests such as IGF-1 and glucose suppression test, supported by imaging. Treatment includes surgery, medical therapy, and newer receptor blockers.
Detailed Questions:
Q1.1: What is the cause of acromegaly?
Answer:
- Pituitary adenoma causing excessive GH production after puberty.
Q1.2: Why does acromegaly not increase height?
Answer:
- Occurs after epiphyseal plate closure post-puberty → no longitudinal bone growth.
Q1.3: What are the clinical features of acromegaly?
Answer:
- Spade-like hands (increase in hand size)
- Prognathism
- Increased foot size
- Increased heel pad thickness
- Galactorrhea
Q1.4: Which anterior pituitary cells are most abundant and involved?
Answer:
- Somatotrophs (main)
- Lactotrophs (also involved)
Q1.5: What is the screening test for acromegaly?
Answer:
- IGF-1 levels (elevated).
Q1.6: What is the investigational gold standard for confirming acromegaly?
Answer:
- Glucose suppression test:
- Normally, 100 g glucose suppresses GH.
- In acromegaly, GH fails to suppress → GH >1 ng/mL.
Q1.87: Which imaging is used for pituitary adenoma?
Answer:
- MRI of the head.
Q1.8: What are the treatment options for acromegaly?
Answer:
- Lanreotide (long-acting somatostatin analog)
- Trans-sphenoidal surgery
- Pegvisomant (GH receptor antagonist for recurrence)
If you’re looking to strengthen your final prep, don’t miss out on Rapid Revision Reignite by PrepLadder. It’s designed to help Medical PG aspirants cover the entire syllabus quickly with concise notes in a Question-Answer format, high-yield MCQs, and expert-led revision videos—perfect for last-minute reinforcement before the exam.
Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Smarter Video Lectures also in हिंglish, Game Changing Qbank, Audio QBank, Structured Notes, Treasures, Mock test for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
Rheumatology
Detailed Questions
Q1.11 Which antibody is most commonly associated with CREST syndrome?
CARDIOLOGY
Detailed Questions
Q2.1: What are the Modified Duke Criteria for IE?
Neurology
Detailed Questions
Q3.7: In which clinical scenario is Tenecteplase given to a stroke patient?
Q3.8: What are the steps in the management of acute ischemic stroke?