Thrombolysis in Acute Ischemic Stroke- NEET PG Medicine
Feb 14, 2023

Thrombolysis in Acute Ischemic Stroke is an important topic for the NEET PG exam because it is a crucial aspect of stroke management. Stroke is a leading cause of death and disability, and prompt and effective treatment is essential for improving outcomes. Thrombolysis, also known as clot-busting therapy, involves the use of drugs to dissolve blood clots and restore blood flow to the brain.
Read this blog further for a quick overview of this important medicine topic.

Radiological Finding
- Non contrast CT head: Normal (in majority cases)
It is done initially not to identify ischemic stroke but to rule out haemorrhagic stroke. One of the side effects seen with thrombolysis is increased incidence of bleeding.
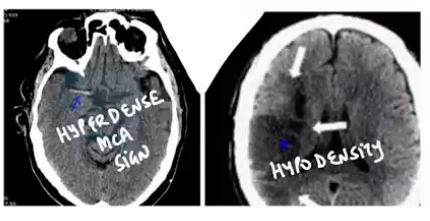
Traditionally with ischemic damage there should be a relatively blackish area i.e., hypodensity but this will take some time to develop. Initially the clot that develops in the middle cerebral artery will appear relatively hyperdense i.e., Hyperdense MCA sign (not encountered in majority of cases). Subsequently damage would show up in the form of hypodensity in patient
Thrombolysis can be done up to 4.5 hours. In America, USA: Thrombolysis is indicated up to 3 hours, in Canada, UK – Thrombolysis is indicated up to 4.5 hrs. Current edition of Harrison says that the benefit can be up to 6 hours. So, thrombolysis can be done upto: 4.5 – 6 hours (upper limit 6 hours). After 6 hours: Mechanical thrombectomy is done. More number of patients that we are able to treat, the more the resultant decrease in residual deficit of patients, the better it is.
| Indications | Contraindications |
| Clinical diagnosis of stroke | Sustained BP > 185/110 mmHg despite treatment (labetalol or nicardipine) |
| Onset of symptoms to time of drug administration ≤ 4.5 hours | Bleeding diathesis (INR > 1.7) |
| CT scan showing no hemorrhage or edema > 1/3 of the MCA territory Age ≥ 18 years | Recent head injury or intracerebral hemorrhage |
| Major surgery in preceding 14 days | |
| GI bleeding in preceding 21 days | |
| Recent myocardial infarction |
- If a person wakes up with symptoms of stroke like if an Indian patient went to bed at 10 p.m. at night and he wakes up with symptoms of stroke then no thrombolysis is done.
- Then the relatives are asked when the patient is seen or heard normally because lots of time old people are staying alone in India in old age homes and their children may be abroad and they might be in contact with them through social media in the form of video call daily.
- So, with the help of their son or daughter by asking when did they speak to their mother or father earlier when they were perfectly normal.
- Window period: 4.5 hours but recently this window period has been slightly extended to increase benefit to a larger number of patients.
Also Read:
Myocardial Infarction - Neet PG Medicine
EPILEPSY AND Electroencephalography (EEG) : NEET PG Medicine
Contraindications
If BP is very high and thrombolysis is done and bleeding occurs then the patient can die.
- Case scenario: A person underwent an aortic aneurysm surgery and postoperatively when he was discharged back home he started developing symptoms of stroke
- So thrombolysis is not done in these patients.
- We can go into that artery where thrombus is while doing CT angiography and subsequently mechanical thrombectomy can be done.
- Where the clot is removed or extracted that was causing physical obstruction of any important blood vessel of the brain.
- Most of the time it is the M1 or M2 part of the middle cerebral artery or starting point of the internal carotid artery.
- Action plan for management of stroke (Harrison 21st edition update)
- Patient who is candidate for thrombolysis (within first 6 hrs)
- Age > 18 years
- A person having no evidence of hemorrhage with respect CT head
- Onset of symptoms (earlier detected/intervened more brain tissue can be saved)
- Drug – Alteplase: Initially bolus subsequently infusion is given
- Tenecteplase: Given right inside CT scanner as a bolus
- Patient with clinical feature suggested of stroke, CT scan normal & rule out evidence of hemorrhage: Tenecteplase given
- Tenecteplase: Given right inside CT scanner as a bolus
- Patients not eligible for thrombolysis i.e., patients with contraindications – Then perform CT angiography
- This CT angiography will evaluate blood vessel that originate from aortic arch right up to middle cerebral artery and basilar arteries
- Carotid artery (Internal carotid artery) originates from left side of aortic arch
- If occlusion of M1 and M2 of middle cerebral artery or basilar artery is determined then mechanical thrombectomy can be done (MERCI: Mechanical embolus retraction in cerebral ischemia). Earlier according to the guidelines given in Harrison – It was a CT scan and then there was no investigation but now after CT scan there is CT angiography. To pick up finding of ischemic stroke early: Diffusion weighted MRI is available
- Ideally there should be plain CT, CT angiography (to give contrast in patient) and then Diffusion weighted MRI. So, the more investigation you have, the more you will be able to diagnose it earlier. In resource limited settings like in India there might be disadvantages there will be plain CT scan. This table incorporates whether there is limited resource setting or whether there is exhaustive resource
- Management in any patient of acute ischemic stroke
- Assess airway
- BP control: Drugs like Nicardipine and labetalol can be used
- Time last seen normally
- Evaluate severity of stroke by NIHSS (National Institute of Health Stroke Severity)
- If NIHSS > 5
- Do thrombolysis
- Endovascular therapy: MERCI
- Once acute ischemic stroke is handled
- Then aspirin can be given after first 24 hours
- It will prevent redevelopment of shock and reduce current mortality
- Ticagrelor: Loading dose 180 mg and subsequently 90 mg twice a day
- Then aspirin can be given after first 24 hours
- Antiplatelet therapy given for STEMI, non-STEMI even in patients of transient ischemic attack and currently in patients of acute ischemic stroke as well. It is demonstrated to reduce mortality. After I month: Ticagrelor will be discontinued and aspirin will be continued low dose for whole life of this patient 75- 81 mg whichever is available (In Harrison: 81 mg)
- D.A.P.T: Aspirin + Ticagrelor should be continued for 1 month, it reduces chances of reinfarction in these patients. Statins for atherosclerosis
- Anticoagulant agents: Apixaban – Atrial fibrillation
- If it is rheumatic heart disease, mitral stenosis then warfarin is given
- If there is atherosclerotic narrowing of internal carotid artery then either in same hospitalisation or may be on later admission carotid endarterectomy can be done. If there is narrow ICA there could be plaque fissure subsequently that will keep on throwing embolic fragments into the brain
- Achieve target systolic blood pressure
- Initially SBP can be 130/140 to ensure cerebral perfusion
- Cerebral perfusion = Mean arterial pressure – intracranial pressure
- But trials have shown if a person has suffered from shock & once he is on road to recovery/ handled the acute phase then subsequently the target of BP in range of 120 or less should be achieved (acc. to updated edition of Harrison). Earlier the clear cut target BP value was not given with respect to someone who has suffered from acute ischemic stroke
For more insightful content that can strengthen your NEET PG exam preparations, download the PrepLadder app.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!