What is Myocardial Infarction ? - NEET PG Medicine
Feb 7, 2023

This article will help you dig deeper into what is Myocardial Infarction, definition of Myocardial Injury And Infarction, and Myocardial Infarction treatment.
Read further to amplify your NEET-PG exam preparation. Let’s get started!
Coronary artery disease contributes to maximum amount of mortality in India. India is anyway the diabetics capital of the world and the no.1 reason why diabetics would be dying is by cardiovascular causes that would be ranging from ST elevation to non-ST elevation, unstable angina. If they are not treated properly the patient would end up with heart failure, severe pulmonary oedema and can die.
Let’s look at the cut section of any one coronary artery: left anterior descending (LAD)/ right coronary artery (RCA)
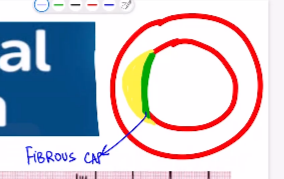
- Yellow here is a fat deposition i.e., lipid core
- Green is the fibrous capsule: Atherosclerosis (contains the lipid core in the middle i.e., in tunica intima and the covering is the fibrous cap)
- When blood is going through this coronary artery at a fixed amount of pressure what really can happen here is, there could be a development of a tear in the luminal surface i.e., plaque fissure.
- And the movement there is going to be a plaque fissure, there would be exposure of collagen right deep inside the blood vessel which will cause the platelet to jump onto the opportunity
- Because of this plaque fissure the platelets would be attracted to collagen and collagen act like the magnet here and very soon there would be a platelet plug formation and then there is going to be a clot formation or thrombus formation
- And this thrombus will occlude the entire lumen of the coronary artery, results in muscle death/ myocardial necrosis in couple of minutes.
- Important Information:
- MI is of 2 varieties:
- STEMI (ST ELEVATION MI)
- NSTEMI (NON -ST ELEVATION MI)
- In STEMI, the clot is rich in Fibrin and RBCs. Therefore, fibrinolytic drugs like Streptokinase, Alteplase, Reteplase, Tenecteplase will work
- In NSTEMI, clot is rich in platelets. Therefore, we use antiplatelet/antithrombotic drugs and don’t use thrombolytics and they are not effective. Therefore, thrombolysis is C/I in NSTEMI

ECG INTERPRETATION
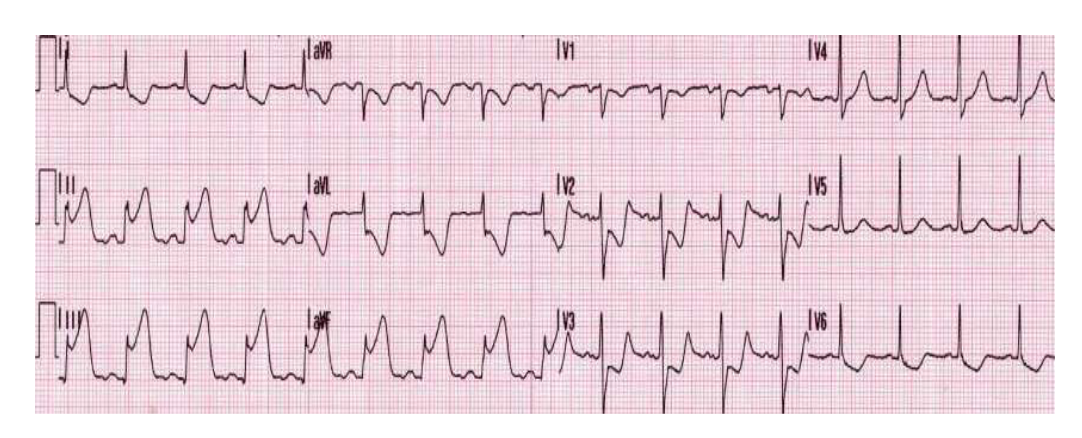
- Most of the time in exam they give question starting with patient presents with chest pain and the ECG image with ST elevation in LEAD II, III, and AVF. In this question you need to calculate HR, and look at the infarct localization i.e., find which surface of the heart is involved
- Important information
- Which leads to look for changes in MI:
- Inferior wall MI: Lead 2, 3, aVF
- Anterior wall MI: Lead 1, aVL, V1 to V4
- Lateral wall MI: V5, V6
- Septal MI: V1, V2
- Inferior surface of the heart is mainly composed of the right ventricle. Some part of RV faces the sternum and majority of the part face the inferior surface i.e., towards diaphragm
- In Inferior wall MI the thrombus mainly presents in RCA
Also Read: What is CONGESTIVE HEART FAILURE ? - NEET PG MEDICINE
ECG Interpretation
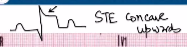
- In lead II: P wave present, no Q wave, characteristic ST elevation present k/a TOMB STONE PATTERN (ST elevation, convex in upward direction)
- Whereas, if ST elevation is present but if it is concave upwards, it is due to inflammation of the outer layer of the heart e.g., Acute Pericarditis.
- In this case to differentiate MI and Acute pericarditis. Cardiac biomarkers like troponin I, troponin T, CPKMB are elevated in MI and usually normal in Acute Pericarditis.
- In chest leads: ST depression is seen in V1,2,3,4
- In this ECG: the characteristic ST elevation in lead II, III, aVF & ST depression in V1,2,3,4 S/O Inferior wall MI
ECG Findings in MI
- In MI there is change in polarity of T wave but no change in PQRS wave
- PQRS wave represent the absolute refractory period of heart
- Even if you stimulate in absolute refractory period there will be no change
- T wave represents the relative refractory period. If you stimulate in relative refractory period changes will be seen.
- Hyper acute T wave (Earliest ECG finding)
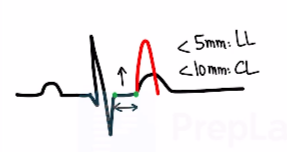
- Normal size criteria of T wave:
- Vertical size is <5mm in limb leads & <10 mm in chest leads
- More than normal size of T wave k/a Hyperacute T wave
- Hyperacute T wave indicates Myocardial Ischemia.
- Will be present within seconds of infarction
- ST elevation
- For significant ST elevation:
- For Male patient: the rise is >/= 2mm.
- For female patient: the rise is >/=1.5mm.
- ST elevation indicates Myocardial injury.
- Myocardial injuries are best identified by cardiac biomarkers
- ST elevation is called as current of injury
- Will be present within minutes of infarction
What is the best test for diagnosis of MI?
Ans: Cardiac bio markers
Because if there is injury to myocardial tissue, cardiac biomarkers (Troponin T, Troponin I) are released from myocytes
Which of the following is called as current of injury?
Ans: ST elevation
- T wave Inversion
- Q waves/ pathological Q waves
- Indicates Cell Death (E.g., Previous MI)
- They are mostly Pathological.
- A deep Q wave persists for whole life.
- Will be present >1hr of infarction
Related Articles :
Definition of Myocardial Injury And Infarction
Criteria for Myocardial Injury
The term myocardial injury should be used when there is evidence of elevated cardiac troponin (cTn) levels with at least one value above the 99th percentile upper reference limit (URL). The myocardial injury is considered acute if there is a rise and/or fall of cTn values.
- Value of troponin I in Kits might vary in different hospitals for e.g., in one of the kits the normal value of trop I is 0.04ng/dl, the minimum value to say the patient is suffering from MI is doubling of the Trop I value. And it indicates the myocardial necrosis has already occurred
- In MCQ, they will mention that troponin (cTn) one value above the 99th percentile upper reference limit (URL)
- Troponin I value is not going to rise immediately
- Troponin I value rise occur in 3 to 4 hrs in contrast with CPKMB which will take about 4 to 6 hrs to rise
- If the patient presents within 1 hr of chest pain the troponin value will be normal in this case the diagnosis of MI can be made by ECG findings. Therefore, ECG is done first but ECG alone should not be used as diagnosis or conformation along with-it cardiac biomarkers are also useful in making diagnosis of MI
- ECG and cardiac biomarkers any of the two is sufficient to make diagnosis and initiate treatment. But most specific is serial troponin I
Also Read: EPILEPSY AND Electroencephalography (EEG) : NEET PG Medicine
Criteria for Acute Myocardial Infarction (types 1, 2 and 3 MI)
The term acute myocardial infarction (MI) should be used when there is acute myocardial injury with clinical evidence of acute myocardial ischemia and with detection of a rise and/or fall of cTn values with at least one value above the 99th percentile URL and at least one of the following:
- Symptoms of myocardial ischemia:
- Levine’s sign is a clenched fist held over the chest to describe ischemic chest pain > 20 mins
- New ischemia electrocardiographic (ECG) changes
- Development of pathologic Q waves
- Imaging evidence of new loss of viable myocardium or new regional wall motion abnormality in a pattern consistent with an ischemic etiology
- Echo shows regional hypokinesia/ stunned myocardium (sudden decrease in the contractility of the heart). The problem in mechanical function is because there is less supply of O2 primarily due to thrombus in anyone of the coronary artery
- Identification of a coronary thrombus by angiography or autopsy (not for types 2 or 3 MIs)
- If the patient is having elevated trop I with any one of the above is present, then it is MI
- Best test/ IOC/ gold standard diagnosis for MI: Elevated cardiac biomarkers with any one of the above 5 points
- Leading cause of death in DM is cardiovascular mortality: Silent MI
Geriatric age patient with DM, HTN presents with chest pain (when there is no diabetic neuropathy chest pain will present) then MI is considered
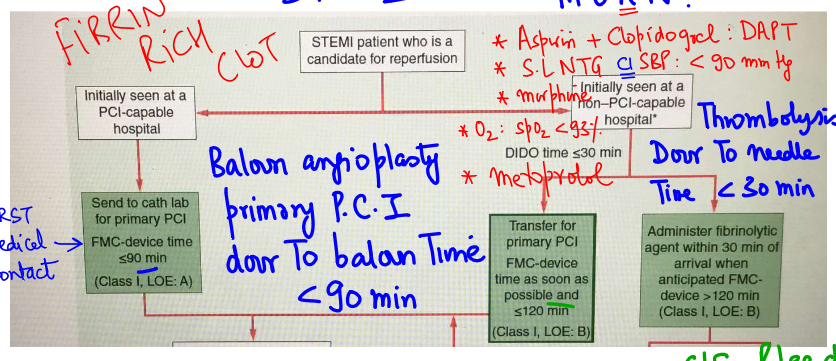
STEMI- MANAGEMENT
Scenario 1
If cath lab facility is available shift patient to cath lab and do coronary angiography by using femoral or radial artery access, but preferred is radial artery access. Guide wire is sent retrogradely by radial artery towards the heart. In the monitor we can see that the contrast is unable to flow forward because of the coronary artery occlusion, in this condition we do balloon angioplasty/ primary percutaneous intervention (PCI)

TOC for STEMI: Primary PCI
Ideal Door to Balloon time is <90 mins
Scenario 2
- If it is non-PCI hospital, we will initiate thrombolysis and that should be started in shortest possible time
- Door to needle time should be <30 mins (for thrombolysis)
- Mnemonic: M O A N (Morphine, O2, Antiplatelet, NTG)
- Dual antiplatelet therapy (DAPT): Aspirin + ticagrelor
- DAPT useful in: STEMI, NSTEMI, Unstable angina, TIA, stroke, stenting in heart, coronary bypass grafting
- Anti-ischemia measure: sublingual nitro-glycerine (SLNTG)
- Avoid SLNTG if SBP is <90 mmHg because SLNTG is a vasodilator further decrease in BP will compromise the coronary blood flow and renal blood flow in hypotension
- Morphine
- Morphine is used when NTG is given 3 times and there is no improvement over a span of 15 mins.
- O2: if SPO2 < 93%
- Inferior wall MI involves RV, RV involvement won’t cause Pulmonary oedema.
- LV involvement will cause Pulmonary oedema that will lead to drop in SPO2 and O2 is required in this condition
- M.O.A.N is the initial procedure to stabilize the patient, once pt reached the hospital betablockers are used
- Beta blockers: metoprolol, it reduces the O2 consumption by decreasing the HR.
- Avoid beta blockers if HR is below 60/min like in heart block
- Metoprolol helps to reduce the size of the infarct by decreasing O2 consumption
- The Upper limit of thrombolysis is <12 hrs. (We are talking about the upper limit, not the optimal time)
- > 12 hrs the side effects of thrombolysis are more than the benefit to the patient
- S/E of thrombolysis: bleeding (like intra cranial bleeding)
- Antidote of streptokinase toxicity: Epsilon Amino Caproic Acid (E.A.C.A)
- Window period of acute ischemic stroke is 4.5 hrs (for thrombolysis)
- Neurons are more susceptible to hypoxia whereas cardiac muscle can resist hypoxia for a relatively longer duration
- Thrombolysis is C/I in haemorrhagic stroke, if thrombolysis is done the bleeding will worsen and the patient will deteriorate.
Also Read: Cardiopulmonary Resuscitation: How to Perform CPR, Types of CPR
Important information
- TOC for STEMI: Primary PCI
- Thrombolysis is C/I: NSTEMI
- STEMI the clot is fibrin rich clot, and it is possible to destroy it by doing thrombolysis
- NSTEMI the clot is platelet rich, when we do thrombolysis the S/E of bleeding is occurring, and the benefit is not occurring. Therefore, Thrombolysis is C/I in NSTEMI
To scale up your NEET PG preparation with the best-in-class video lectures, QBank, Mock Tests and more, download the PrepLadder App!
Download PrepLadder's NEET PG preparation app for Android
Download PrepLadder's NEET PG preparation app for iOS
Stay tuned for more exam preparation articles and updates!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
ECG INTERPRETATION
ECG Interpretation
ECG Findings in MI
Definition of Myocardial Injury And Infarction
Criteria for Myocardial Injury
Criteria for Acute Myocardial Infarction (types 1, 2 and 3 MI)
Scenario 1
TOC for STEMI: Primary PCI
Ideal Door to Balloon time is <90 mins
Scenario 2
Important information
Top searching words
The most popular search terms used by aspirants
- NEET PG Exam Tips
- NEET PG Medicine
- NEET PG Preparation