What is Pneumonia? - NEET PG Medicine
Feb 15, 2023

Pneumonia is a common respiratory illness and a leading cause of morbidity and mortality worldwide, especially in young children and elderly individuals. It is a common presentation in clinical practice, and medical professionals need to be familiar with its management, including the use of antibiotics, and supportive care.
Read this blog for a quick overview of this important medicine topic for NEET PG exam Preparation.

Overview
- Commonest cause for community acquired pneumonia is Pneumococcus
- Pneumonia in AIDS +ive patient, low CD4 count of <200 cells / cu.mm
- Opportunistic infection in AIDS +ive patient is Pneumocystis jirovecii
- Case 1: AIDS positive truck driver with pneumonia and low CD4 count. He is having bronchial breathing and lobar consolidation
- Lobar consolidation and bronchial breathing are absent in pneumocystis jirovecii,
- If bronchial breathing and Lobar consolidation are given in question, the answer is Pneumococcus. Because the leading cause of Pneumonia in AIDS positive patients is Pneumococcus.
- Low CD4 count is s/o pneumocystis jirovecii but not confirmatory.
- Conformation of Pneumocystis jiroveci is done by Bronchoalveolar Lavage stained with gomori methenamine silver stain and black cysts of Pneumocystis jiroveci are seen.
- The word pneumocystis means the cysts causing pneumatocele in Lungs.
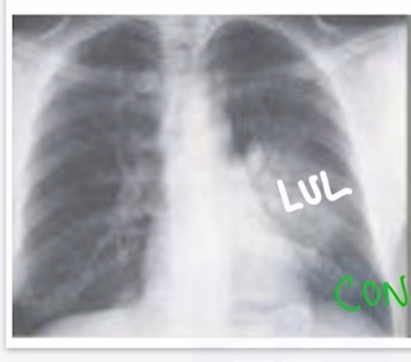
- Below X-ray shows Lobar consolidation in Left upper lobe.
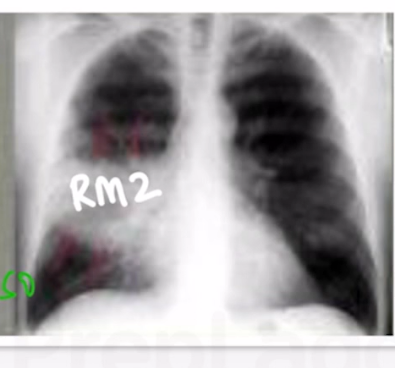
- Below X-ray shows Lobar consolidation in the right middle zone.
| Important information MC organism for acute bacterial meningitis in adult and pediatric population is Pneumococcus |
Also Read: Myocardial Infarction - Neet PG Medicine
Pneumocystis jirovecii
- Pneumocystis jirovecii causes interstitial pneumonia.
- Chest is clear initially, later develops diffuse rales
- Chest X-ray: Bilaterally symmetrical perihilar reticular interstitial changes are seen
- HRCT chest: Diffuse ground glass opacities
- LDH increases.
- Increase A -a gradient.
- Confirmatory test: BAL stained with gomori methenamine silver stain which demonstrates the cysts.
- Rx: TMP - SMX (DOC for treatment and prevention)
- Other drugs: Pentamidine, Clindamycin, Primaquine, Atovaquone, steroids.
| Important information In covid -19 pneumonia HRCT shows ground glass opacities & D-Dimer increases. Confirmatory test for covid-19: RTPCR. Steroids used in both covid-19 and Pneumocystis Jiroveci causing interstitial pneumonia. |
| Important Information Commonest cause of pneumonia in AIDS positive patient is Pneumococcus not Pneumocystis jivovecio |
Organism Specific Approach for Pneumonia
- Alcoholism= S. pneumonia, Klebsiella Pneumoniae, oral anaerobes.
- Klebsiella pneumonia in alcoholics causes Necrotizing Pneumonia that results in a feature of red currant Jelly sputum.
- Oral anaerobes in alcoholics cause Necrotizing Pneumonia that results in lung abscess. Chest X-ray showing air fluid level S/O Lung abscess
- Impaired airway defence seen in alcohol/drug intoxication, dementia, stroke, etc., cause of pneumonia is Oral anaerobes
- Rx of oral anaerobes causing Pneumonia is clindamycin
| Important information 1. Red currant Jelly stool in 9-month baby S/O intussusception 2. Multiple air fluid level in X-ray abdomen S/O Intestinal obstruction |
- COPD: H. influenzae
- Lung abscess: oral Anaerobes? Primary.
- CA-MRSA ? Secondary to setting of foreign body, Tumor, Infection.
- Hotel stay / cruise : Legionella Pneumophila. (due to inhalation of water droplets)
- Infected Humans: SARS - COV 2
- Birds: H. capsulatum, C.pittaci
- Rabbits: F. tularensis.
- Tularemia is caused by the bacterium Francisella tularensis.
- Hunter after killing a rabbit develops Eschar/ ulcer and regional lymph node swelling.
- Ulceroglandular fever: The most common form of tularemia and usually occurs following a tick bite or after handing of an infected animal. The ulcer is accompanied by swelling of regional lymph glands, usually in the armpit or groin.
- Sheep: Coxiella Brunetti / Q fever
- Coxiella Brunetti cause atypical pneumonia and Endocarditis as well.
Rx of Atypical Pneumonia: Macrolides.
Clinical feature Points Confusion (defined as a Mental Test Score of ≤8, or disorientation in person, place, or time ) 1 Uremia: BUN >7 mmol/L ( ~19 mg / dL) 1 Respiratory rate: ≥30 breaths / minute 1 Blood pressure: systolic <90 mm Hg or diastolic ≤60 mm Hg 1 Age ≥65 years 1 Total points
- BUN = UREA/2.14
- E.g., BUN= 10, UREA = BUN x 2.14 = 10 x 2.14 = 21.4 mg/dl
- Urea = BUN x 0.35
- E.g., BUN= 10, Urea = 10 x 0.35 = 3.5 mmol/L
| Treatment options based on CURB -65 Score | ||
| Score | Group | Treatment Options |
| 0 | Group 1; mortality low (1.5%) | Low risk; consider home treatment |
| 1-2 | Group 2; mortality intermediate (9.2%) | Consider hospital-supervised treatment (either short – stay inpatient or hospital – supervised outpatient) |
| 3 | Group 3; mortality high (22%) | Manage in hospital as severe pneumonia; consider admission to |
- For group 1: OPD management is done
- For group 2: IPD management is done. E,g., 70 yrs old patient with elevated BUN RX: IV Augmentin with macrolides
- For group 3: ICU management is done
- If only age is >/= 65 and rest are normal. Treatment is based on health condition of patient the treating doctor can decide the type of management.
- If age along with another deranged parameter is given. Then admit patient and give parenteral antibiotics
Also Read: EPILEPSY AND Electroencephalography (EEG) : NEET PG Medicine

Treatment Strategy For C.A.P
- For outpatient management
|
Treatment strategy: C.A.P: outpatient |
|
|
No comorbidity
|
Comorbidity or Rcvd A/b in lost 3 months
|
For Inpatient Management
- Beta lactam+ macrolide or respiratory fluroquinolones (levofloxacin, moxifloxacin, Gemifloxacin)
- If recent hospitalization/ respiratory isolation
- Add coverage for MRSA: Vancomycin/ linezolid & for pseudomonas: Piperacillin-Tazobactum
To study this topic in detail, head over to the PrepLadder app and find engaging video lectures covering the entire topic comprehensively.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Overview
Pneumocystis jirovecii
Organism Specific Approach for Pneumonia
Rx of Atypical Pneumonia: Macrolides.
Treatment Strategy For C.A.P
For Inpatient Management
Top searching words
The most popular search terms used by aspirants
- NEET PG Medicine
- NEET PG Preparation