Fibroid Uterus: Causes, Symptoms, Diagnosis & Treatment
Aug 2, 2023

A fibroid uterus is a noncancerous uterine growth that frequently manifests itself while a woman is pregnant. Uterine fibroids, also known as leiomyomas or myomas, don't enhance the risk of uterine cancer and hardly ever turn cancerous.
Fibroids differ in size from tiny, visually invisible seedlings to big, obtrusive masses that can stretch and expand the uterus. One fibroid or more may exist in your body. In severe conditions, there can present numerous fibroids which can cause the uterus to enlarge to the point where it touches the rib cage and puts pressure.
Uterine fibroids are extremely common in women. However, uterine fibroids frequently do not show any symptoms so you might not be aware that you have them. During a pelvic exam or prenatal ultrasound, your doctor can unintentionally find fibroids.

Causes and Risk Factors Of Fibroid Uterus
Below are mentioned some of the risk factors and causes of fibroid uterus:
- Fibroids are seen in as many as 30% of all women. This incidence rises to about 80% in women of age more than 50 years.
- A woman is 2.5 times more likely to get affected if one female relative has fibroid.
- Associated with a chromosomal abnormality in 40% such as 12-14 Translocation, 12 Trisomy, and 7 deletion
- Seen in nulliparous women
- Associated with an increase in Estrogen & Progesterone
- Obese women
- Red meat eaters
- Increase in the Growth Factors such as:
- Transforming growth factor β
- Platelet-derived growth Factor
- Epidermal growth Factor
- Vascular Endothelial Growth Factor (VEGF)
Pathology Of Fibroid Uterus
Fibroids are monoclonal smooth muscle cell tumors, they always start in the intramural area of the muscle layer like Whorls of smooth muscle cells surrounded by pseudo capsules. This fibroid present in the intramural area is treated as a foreign body by the uterus. The uterus responds by contracting to push the fibroid either outwards (subserosal fibroid) or inwards (submucosal fibroid)
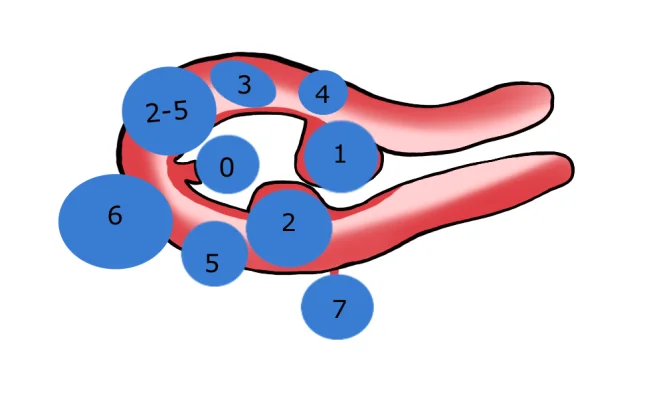
Figo Classification
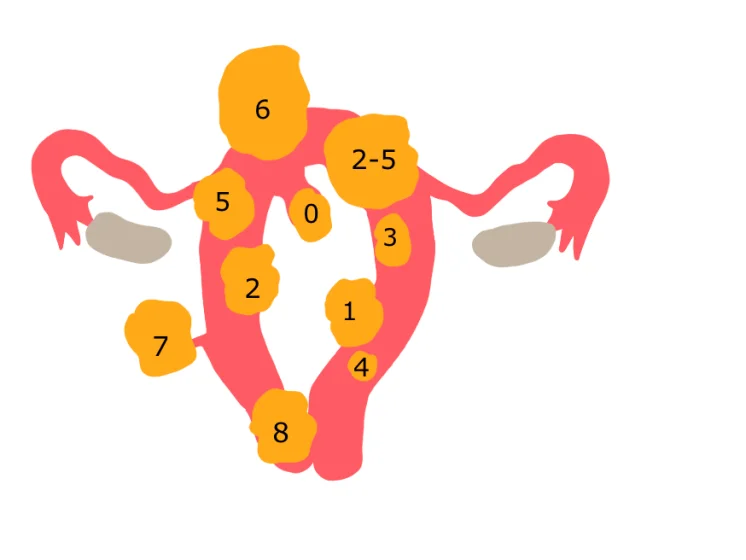
- Type 4: Intramural
- Type 3: 100% intramural but touches the cavity.
- Type 2: >50% intramural and a part in cavity or submucosal.
- Type 1: <50% intramural and rest in cavity
- Type 0: Pedunculated or intracavitary or submucosal
- Type 5: >50% intramural and rest in serosa (subserosal)
- Type 6: <50% intramural and rest in serosa (subserosal)
- Type 7: Subserosal Pedunculated
- Type 8: Parasitic fibroid (Detached fibroid that may be stuck to the diaphragm or omentum) and cervical fibroid.
- Type 2-5: Part of the fibroid is present both in the cavity (Type 2) and in the serosa (Type 5) and this is known as Hybrid Fibroid




Diagnosis of Fibroid Uterus
Fibroid uterus can be diagnosed with the help of the following methods:
- USG
- MRI is the best imaging technique for fibroids and is also used for fibroid mapping.
- Endometrial biopsy must be done to rule out endometrial hyperplasia which occurs due to increased estrogen.
.jpg)
Treatment Of Fibroid Uterus
Following are mentioned some of the treatment options for fibroid uterus:
- A small fibroid of less than 5cm without pain, bleeding, or infertility requires no treatment, however, if there is pain or bleeding, or infertility, then treatment is required.
- Large fibroid of more than 10 cm with or without pain or bleeding or infertility requires treatment as an asymptomatic large fibroid may undergo torsion, compaction, degeneration, compression of bladder and bowel or it can detach (parasitic fibroid).
Medical Management
- NSAIDS reduce pain & bleeding.
- Tranexamic acid reduces bleeding.
- GnRH analogs (Leuprolin, Goserlin) cause downregulation of the pituitary, such that no FSH or LH is made, causing amenorrhea. These drugs reduce the size and vascularity of fibroid, therefore are beneficial when given prior to surgery, to minimize blood loss.
- GnRH antagonists (cetrorelix, ganirelix) cause direct suppression of pituitary and amenorrhea.
- Mifepristone acts as an “Anti-growth” (anti-progestin) agent for fibroid growth.
- Ulipristal is a selective progesterone receptor modulator and has pure antagonist action on progesterone receptors in the uterus.
Newer Methods
- Uterine artery embolization with PVA particles (Poly Vinyl Alcohol) and preferably >35 years
- HiFU: High-Frequency Focused USG
- MRgFUS: MR guided focused USG
- Intrauterine progesterone devices (MIRENA – levenergosterol IUCD) result in atrophy of the endometrium
- Myolysis needle: Electrocautery or laser needle is used to cause lysis of muscle.
Also Read :
Vaginal Prolapse: Causes, Symptoms, Risk Factors, Diagnosis and Treatment
Surgical Management
- Hysterectomy for patients who completed family and can be done either by open technique or laparoscopy.
- Myomectomy is preferred for those planning pregnancy. The open technique may be used for any size, while Laparoscopic myomectomy, which is a more skilled procedure, may be done for smaller fibroids. Criteria for laparoscopic myomectomy include 3-4 fibroids with size < 5cm or one fibroid < 15 cm can be removed. It is preferred for types 7, 6, 5 .
Pre-Requisites for Myomectomy
- Hb > 10 gm
- Normal semen analysis
Techniques for reducing blood loss
- Pre-operative GnRH therapy
- Intra-op use of Uterine clamp, Tourniquet, and Injection of vasopressin (Pitressin)
- Minimal fimbrial tube handling
- The minimal incision on the uterus
- Avoid posterior uterine wall incision → fixed retroversion leading to infertility
- Avoid opening the cavity
Criteria for Hysteroscopic Myomectomy
- Fibroid inside the uterus with a size < 3cm
- Type 1, 0, or even type 2 fibroids can be removed
- Distention of the uterus using fluids may be required for visualization and manipulation.
- Fluid can escape into the peritoneal cavity or into circulation. Hence fluid deficit should be monitored
| Warning | Stop the Sx | |
| Non-electrolyte media (glycine) | 500-750ml | > 1500ml |
| Electrolyte media (saline) | 1000ml | 2500ml |
- Glycine (non-conducting media) can be used with unipolar current
- Ionic solution (conducts electricity) used with bipolar current
Side effects of fluid overload in operative hysteroscopy
- Pulmonary edema
- Cerebral edema
- Cardiac failure
- Hyperammonemia (glycine)
- Hyponatremia
- Death
Download the PrepLadder App and get the best neet pg online coaching with world-class video lectures, QBank, Mock Tests and more!
Download PrepLadder's best app for neet pg preparation for Android
Download PrepLadder's best app for neet pg preparation for ios

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Causes and Risk Factors Of Fibroid Uterus
Pathology Of Fibroid Uterus
Figo Classification
Diagnosis of Fibroid Uterus
Treatment Of Fibroid Uterus
Medical Management
Newer Methods
Surgical Management
Top searching words
The most popular search terms used by aspirants
- Gynecology OBGYN
- NEET PG OBGYN