Obstetrics and Gynecology NEET PG - Ultrasound
Jun 6, 2026
Key concepts, indications, and important imaging findings
We will explore a clinical case that will distinguish the best rankers from the others. Imagine a 28-year-old primigravida in her 12 weeks. She’s there for her first-trimester screening. The nuchal translucency is 4.2 mm as shown by the ultrasound. Her blood test reveals a drop in serum PAPP-A, and the free beta-hCG is highly increased.
The examiner will present you with the following question: What do you think is the probable chromosomal problem in this case, and what is your next clinical action?
When you can name Trisomy 21 and provide chorionic villus sampling in less than ten seconds, you have understood how obstetric imaging is a high-yield mark-winner. This isn't just one subject; it’s the crossroads where Radiology, OBG, and Pediatrics meet.
The Quick Answer
Obstetric ultrasound is a non-invasive, real-time tool. It involves sound waves of 3.5 to 7.5 MHz to monitor fetal anatomy and development during the three trimesters. You must keep in mind the hard limit of Nuchal translucency: 11 weeks -13 weeks 6 days (CRL 45 -84 mm). Your red flag is anything 3.0 mm or more. Crown-rump length is the gold standard parameter when it comes to dating a pregnancy in the first trimester.

Why This is Important to 2026.
Approximately 3-5 direct questions per paper. The examiners have shifted to vignettes that are image-based. They won't just ask for a fact; they’ll show you a Doppler waveform or an anomaly scan marker and ask for your management plan.
In This Post:
- Obstetric Ultrasound Physics & Basics
- Signs in the Trimesters.
- First Trimester: Dating, Viability & NT Screening
- Second Trimester: 18-20 Week Assessment.
- Third Trimester: Growth, Doppler & Wellbeing.
- Gynecological Ultrasound findings
- Doppler Assessment: What you are to measure.
- Gynecological vs Obstetric Breakdown.
- High-Yield Points for NEET PG
- Frequently Asked Questions
What Is Obstetric Ultrasound?
This is fundamentally a real-time imaging method. It is an ionizing radiation-free method of visualizing the fetus, placenta, and uterine environment using sound waves (3.5-7.5 MHz). The absence of radiation is precisely the reason why it is our main weapon in pregnancy, as opposed to CT or regular X-rays.
Physics is a simple feedback loop: a transducer sends out sound waves that reflect off tissue interfaces. These echoes are reflected back and are processed into a grayscale image. You must know the appearance of these interfaces.
Sound is perfectly transmitted through fluid, which is black or anechoic. Dense structures such as bone are very reflective of sound and appear white or hyperechoic.
Download FMGE Previous Year Question Papers PDF For Free
Two types of probes are typically pointed out by our team.
- The transabdominal probe (3.55 MHz) has a lower frequency to penetrate deeper, which you require in the second and third trimesters.
- The transvaginal probe (5-7.5 MHz) has a higher frequency, which provides more resolution, and thus it is the probe of choice in early pregnancy and gynecological practice. It’s always a trade-off: higher frequency gives you a sharper image but loses the depth. A 6-week pregnancy would be TVS, and a 30-week growth scan would be transabdominal.
According to the ACOG, these exams are categorized as standard, limited, or specialized depending on the purpose of your scan and the depth of the scan.
Also Read: FMG June Exam Date ‘26–Eligibility Criteria, Exam Pattern and Preparation Tips
Ultrasound indications: A Trimester-Wise Guide.
First Trimester (Up to 13⁺⁶ Weeks)
The priorities here are to ensure that the pregnancy is in the uterus, viability by cardiac activity, and an accurate date by CRL. This is also the time when we exclude ectopic pregnancies and do NT measurements. Keep in mind the level of discrimination: a gestational sac should be seen on TVS when serum beta-hCG reaches 1,500-2,000 mIU/mL. When the uterus is empty above that level, begin to suspect an ectopic pregnancy.
Second Trimester (14-28 Weeks)
The "Level II" or targeted anomaly scan happens between 18 and 20 weeks. We systematically evaluate the head, face, spine, heart, abdomen, and limbs. Placental location and cervical length are also checked at this time. This scan is intended to detect most of the structural problems, including neural tube defects and skeletal dysplasias.
Third Trimester (28-40 Weeks)
The emphasis is placed on monitoring growth through biometry, the amniotic fluid volume, and placental well-being. The 2024 ISUOG guidelines suggest regular evaluation of biometry and uterine artery Doppler at this stage to maintain a watch on the high-risk cases.
Also Read: FMG June Exam Date ‘26–Eligibility Criteria, Exam Pattern and Preparation Tips
First Trimester: Dating, Viability & NT Screening.
At least one direct question is created each year in this section.
Gestational Age Assessment
The most accurate method of dating a pregnancy is by crown-rump length. It is within 3 to 5 days when measured between 7 and 13 weeks. The accuracy decreases with the course of pregnancy. In the third trimester, you have a margin of error of about 3 weeks.
Mentorship Pearl: During our 10 years of mentoring, we always advise students that when there is a gap of over 7 days between LMP dating and 1st-trimester CRL dating, then you have to follow the ultrasound date.
Viability Milestones
The sure indication of viability is the fetal cardiac activity. You are supposed to observe cardiac activity on TVS when the CRL is 7 mm. When it is 7 mm or above and silent, then you are dealing with a missed abortion. Similarly, if the gestational sac diameter is 25 mm or more but there is no embryo, it's an anembryonic pregnancy or blighted ovum.
- Gestational sac: Can be seen at 4.5-5 weeks.
- Yolk sac: This is the first structure that is seen in the sac at 5-5.5 weeks.
- Fetal pole and heartbeat: Can be seen at 6-6.5 weeks.
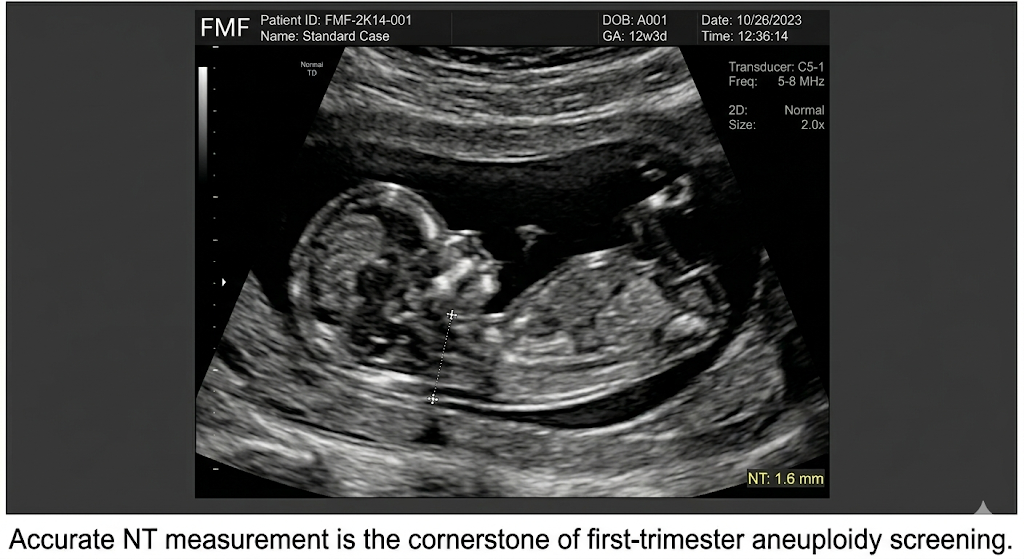
Nuchal Translucency (NT) Details.
NT is the fluid that gathers in the back of the fetal neck. The timing - 11 weeks to 13 weeks 6 days - cannot be negotiated. Measure too soon, and the baby is too small; measure after 14 weeks, and the fluid has already been reabsorbed. The critical level is an NT of 3.0 mm or more.
Combined screening consists of NT + free beta-hCG + PAPP-A. This combo catches about 90% of Trisomy 21 cases. The technique is frequently tested by examiners: with the neck in the neutral position, calipers on the inner borders. You must be able to tell the amniotic fluid apart from the fetal skin.
Also Read: FMGE 2026: Application Process, Important Dates & Documents Required for FMG Examination

The 18-20 Week Anomaly Scan
It is the most elaborate routine scan you will do.
Anatomy Checklist
You have to be systematic. The scan is performed on the head (BPD, ventricles, cisterna magna, cavum septum pellucidum), face (nasal bone, lip integrity), spine, heart (four-chamber and outflow tracts), abdominal wall, and all four limbs.
Soft Markers of Aneuploidy.
These are discoveries that are not anomalies in themselves but increase the danger of chromosomal problems.
- Nuchal fold thickness: More than 6 mm at 15-20 weeks. This is the best indicator of Down syndrome in the second trimester.
- EIF (Echogenic intracardiac focus): A bright spot in the ventricle.
- Echogenic bowel: Bowel as white as bone. Cystic fibrosis, CMV, and Trisomy 21.
- Pyelectasis: Renal pelvis 4 mm or more.
- Choroid plexus cysts: Closely associated with Trisomy 18 (Edwards syndrome).
We highlight the hierarchy in our teaching: nuchal fold > echogenic bowel > EIF > short femur as a risk factor of Trisomy 21.
Third Trimester: Growth & Wellbeing
Biometry
We estimate weight using BPD, head circumference, abdominal circumference (AC), and femur length. The most sensitive marker of catching IUGR is the abdominal circumference. When the AC crosses percentile lines downwards on serial scans, the fetus is not developing correctly.
Amniotic Fluid
- AFI: Sum of deepest pockets in four quadrants. Normal is 5-25 cm.
- Oligohydramnios: AFI < 5 cm. (Mnemonic: DRIP - Drugs, Renal agenesis, IUGR, PROMs).
- Polyhydramnios: AFI more than 25 cm. Associated with esophageal atresia or gestational diabetes.
Placental Grading
Maturity is followed by the Grannum Classification (0 to III). A Grade III placenta before 34 weeks of gestation is regarded as premature aging and is associated with IUGR and hypertension.
Gynecological Ultrasound Indications
Ectopic Pregnancy
The results are an empty uterus with high hCG, an adnexal mass (tubal ring sign), and free fluid in the pouch of Douglas. You must differentiate between a real sac and a so-called pseudogestational sac, which does not have a yolk sac or embryo.
Ovarian Masses & Endometrium
Simple cysts are typically harmless. Complex cysts have septations or solid parts. Dermoid cysts present the "dermoid mesh" or the tip of the iceberg appearance.
In the case of the endometrium, the 4 mm rule is crucial: in a postmenopausal bleeding woman, a biopsy is necessary to exclude cancer when it is more than 4 mm.
Doppler Ultrasound: The High-Risk Patient.
Doppler is a primary IUGR and pre-eclampsia surveillance.
- Uterine Artery: Examined at 20-24 weeks. The presence of a bilateral diastolic notch is a sign of poor trophoblastic invasion.
- Umbilical Artery: The initial option of IUGR. Deterioration appears as follows: higher resistance → absent end-diastolic flow (AEDF) → reversed end-diastolic flow (REDF). REDF is a bad omen of imminent fetal death.
- MCA Doppler: Fetal anemia (PSV > 1.5 MoM) and IUGR (brain-sparing effect). The cerebroplacental ratio (CPR) below 1 is a strong predictor of compromise.
- Ductus Venosus: No a-wave in this case indicates heart failure. This is usually the last parameter to go bad.
Obstetric vs Gynecological Breakdown.
Feature Obstetric Ultrasound Gynecological Ultrasound Primary Probe Transabdominal (TAS) Transvaginal (TVS) Main Goal Fetal development and anatomy Pelvic masses and bleeding Dating Role High (CRL is most accurate) N/A Doppler Context Umbilical artery and MCA Ovarian mass vascularity Key Benchmark AC to detect IUGR 4 mm endometrial thickness
High-Yield Points for NEET PG
- NT is measured at 11-13⁺⁶ weeks. Values ≥ 3.0 mm are abnormal.
- CRL is the most precise dating tool (± 3-5 days).
- The most sensitive IUGR marker is AC.
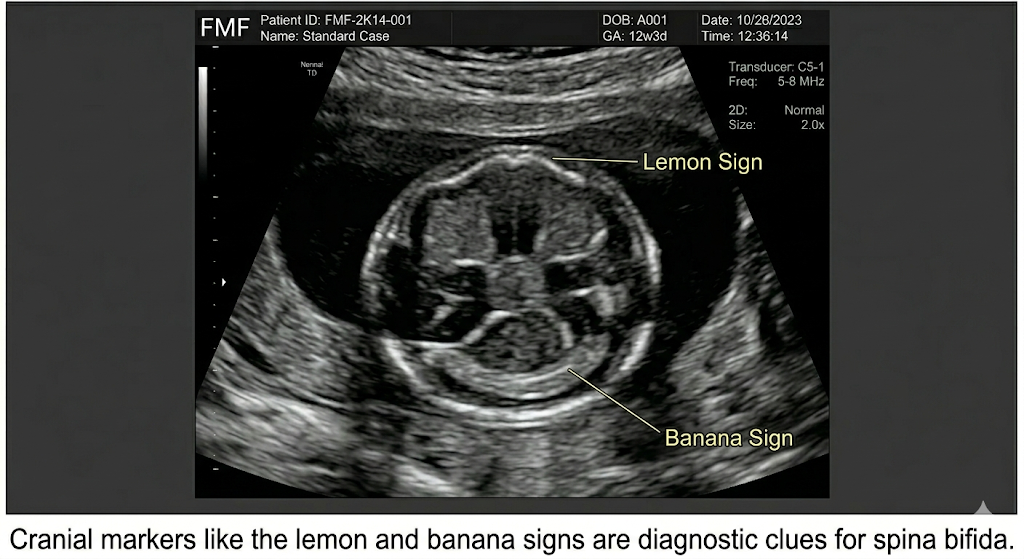
- Lemon and Banana signs = spina bifida.
- Duodenal atresia = double bubble sign.
- Discriminatory hCG: No sac on TVS over 1,500 - 2,000 = suspect ectopic.
- Umbilical Doppler: REDF is the most dangerous stage.
- MCA PSV > 1.5 MoM has replaced cordocentesis for anemia screening.
- NT (1st trimester) is not to be confused with Nuchal Fold (2nd trimester, > 6 mm).
- Choroid plexus cysts = Trisomy 18 link.
- Polyhydramnios mnemonic: Too much fluid = can't swallow or too much sugar.
Frequently Asked Questions
Q1. What is the optimal time to scan the NT?
Strictly between 11 weeks 0 days and 13 weeks 6 days. The baby is too small before 11 weeks; the fluid is reabsorbed naturally after 14 weeks.
Q2.What is the best ultrasound parameter to date?
Crown-rump length (CRL) of 7-13 weeks. Subsequently, the accuracy decreases to ± 5 days to ± 2-3 weeks.
Q3. What is the meaning of AEDF on a Doppler?
The absence of end-diastolic flow implies a high placental resistance, which is typical of severe IUGR. In case it is reversed (REDF), the threat of stillbirth is severe.
Q4. When should I worry about endometrial thickness?
Any bleeding in a postmenopausal patient should be subjected to a biopsy to rule out carcinoma, and anything more than 4 mm is considered abnormal.
Q5. What is the double bubble sign?
There are two fluid pockets in the abdomen of the fetus (stomach and duodenum). It is duodenal atresia, and you will find it in 30% of Down syndrome cases.
Q6. What does the exam test?
Clinical vignettes requesting the next best investigation or image-based questions in which you are expected to interpret a Doppler wave or a fetal cranial sign are expected.
Clinical Pearl
In obstetric ultrasound, time is of the essence - NT at 12, anomaly scan at 20, growth scan at 32. You miss the window, you miss the diagnosis.
Our team can tell you after 10 years of correlating these findings with exam patterns: it is equally important to know when to scan as it is to know what you are looking for. NEET PG tests both.
Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Video Lectures also in हिंglish, digital notes, QBank, and Mock Tests for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
Why This is Important to 2026.
What Is Obstetric Ultrasound?
Download FMGE Previous Year Question Papers PDF For Free
Two types of probes are typically pointed out by our team.
Ultrasound indications: A Trimester-Wise Guide.
First Trimester (Up to 13⁺⁶ Weeks)
Second Trimester (14-28 Weeks)
Third Trimester (28-40 Weeks)
First Trimester: Dating, Viability & NT Screening.
Gestational Age Assessment
Viability Milestones
Nuchal Translucency (NT) Details.
The 18-20 Week Anomaly Scan
Anatomy Checklist
Third Trimester: Growth & Wellbeing
Biometry
Amniotic Fluid
Placental Grading
Gynecological Ultrasound Indications
Ectopic Pregnancy
Ovarian Masses & Endometrium
Doppler Ultrasound: The High-Risk Patient.
Obstetric vs Gynecological Breakdown.
Frequently Asked Questions
Q1. What is the optimal time to scan the NT?
Q2.What is the best ultrasound parameter to date?
Q3. What is the meaning of AEDF on a Doppler?
Q4. When should I worry about endometrial thickness?
Q5. What is the double bubble sign?
Q6. What does the exam test?
Clinical Pearl
Top searching words
The most popular search terms used by aspirants
- NEET PG OBSGYN Preparation
- OBGYN Preparation NEET PG