Rapid Revision Reignite Ophthalmology: Question-Answer Format
Sep 18, 2025

Glaucoma
Big Question 1: What is Glaucoma? What are the modalities used in the management of glaucoma?
Broad Answer:
Glaucoma is damage to the optic nerve by the effect of raised intraocular pressure on the optic nerve head.
- The primary goal of glaucoma treatment is to prevent the progression of visual field defects while maintaining quality of life.
- Medical treatment involves topical drugs: Beta-blockers , Alpha-agonists, Miotics Prostaglandin analogues , Topical CA inhibitors , and RHO Kinase inhibitors
- Systemic drugs include oral CA inhibitors and hyperosmotic agents
- Laser treatment includes Peripheral Iridotomy and Laser Iridoplasty with NdYAG.
- For open angle, Trabeculoplasty is performed.
- For absolute glaucoma, ciliary body ablation damages ciliary processes.
- Surgical treatments are non-penetrating or penetrating, and MIGS.
Detailed Questions
Q1.1: What are the examples, mechanisms of action, and contraindications of drugs used in the management of glaucoma?
Answer:
| Drug Class | Mechanism of Action | Contraindication / Side Effects | Example Drugs / Notes |
| 1. Beta-blockers | ↓ Formation of aqueous | - C/I in asthma- Timolol causes nasolacrimal duct obstruction | - Timolol- Selective: Betaxolol PYQ: INICET 2022, FMGE 2019 |
| 2. Alpha-agonists | ↑ Drainage + ↓ Aqueous formation | - Brimonidine C/I in children (CNS depression)- Adrenaline: conjunctival pigmentation | - Brimonidine (Selective)- Apraclonidine (Selective) |
| 3. Miotics | ↑ Trabecular outflow | C/I in Uveitis | - Pilocarpine |
| 4. Prostaglandin analogues | ↑ Uveal scleral outflow | C/I in Uveitis | - Latanoprost- Travoprost- Isopropyl- Bimatoprost ↑ both outflows |
| 5. Topical CA inhibitors | ↓ Formation of aqueous | C/I in Sulpha allergies | - Dorzolamide- Brinzolamide |
| 6. RHO Kinase inhibitors | ↑ Trabecular outflow | Can lead to Vortex Keratopathy (whorl-like drug deposition) | - Netarsudil |
Q1.2: What are the side effects of topical Latanoprost and adrenaline?
Answer: Latanoprost causes heterochromia iridis (iris pigmentation) due to melanin deposition. Conjunctival pigmentation is caused by adrenaline/epinephrine.
Q1.3: What is "Vortex Keratopathy," and which glaucoma drug causes it?
Answer: Vortex keratopathy (VK) is a side effect of Netarsudil, causing drug deposition in a whorl-like manner. Other causes include Chloroquine, Amiodarone, Tamoxifen, Indomethacin, and Fabry disease.
Q1.4: Which laser is used for Peripheral Iridotomy, and for what condition is it indicated? For Plateau Iris, what laser treatment is performed?
Answer: NdYAG laser is used for peripheral Iridotomy, indicated for angle closure. For Plateau Iris, Laser Iridoplasty is done.
Q1.5: What is the purpose of Trabeculoplasty in open-angle glaucoma? Name three ways it can be performed.
Answer: Trabeculoplasty applies a coagulative laser to the trabecular meshwork to improve aqueous outflow. It can be given in three ways:
- Argon Laser Trabeculoplasty (ALT)
- Selective Laser Trabeculoplasty (SLT) (using yellow NdYAG)
- Micropulse Laser Trabeculoplasty (MLT).
Q1.6: What is the treatment of choice for Absolute Glaucoma?
Answer:
- The treatment of choice is ablation of the ciliary body (Cyclophotocoagulation).
- It works by damaging the ciliary processes to reduce aqueous formation and control pressure.
- Cyclotherapy can be Cryotherapy or Laser photocoagulation.
- It is a diode laser known as DLCP (Diode Laser Photocoagulation).
Q1.7: List two types of non-penetrating surgical procedures for glaucoma.
Answer: Deep Sclerectomy and Viscocanalostomy.
Q1.8: What is the main penetrating surgical procedure for glaucoma?
Answer:
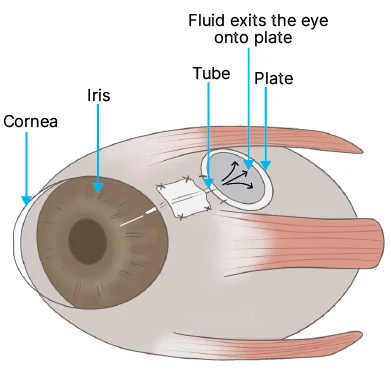
- Trabeculectomy.
- Drugs: Mitomycin C and 5-fluorouracil.
- Implant: Express implant (Titanium)
- Ahmed Glaucoma Valve.
Q1.9: What is "MIGS"?
Answer: MIGS stands for Minimal Incision Glaucoma Surgery.
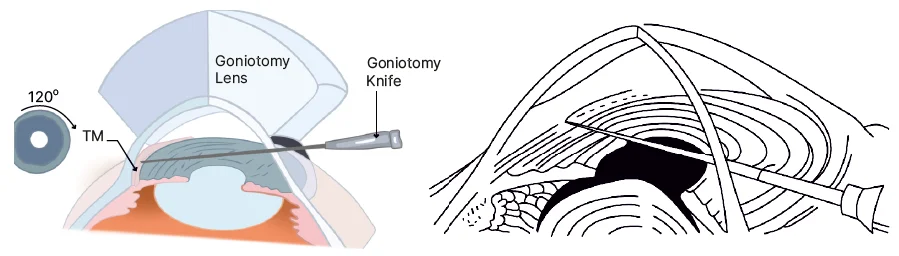
Q1.10: What surgical procedure is the treatment of choice for Congenital Glaucoma, and what instrument is used?
Answer: Goniotomy, done with a Goniotomy knife.
Also Read : Glaucoma Important Questions with Answers
Lacrimal Drainage System
Big Question 2: What is the anatomy, function, disorders, and diagnostic approach related to the lacrimal drainage system?
Broad Answer: The lacrimal drainage system channels tears from the eye surface into the nasal cavity via a defined anatomical path. Disorders like lacrimal obstruction cause watering (epiphora) or discharge due to stagnation. Investigations include the regurgitation test, syringing, and imaging, like dacryoscintigraphy.
Detailed Questions
Q2.1: What is the anatomical pathway of tear drainage?
Answer:
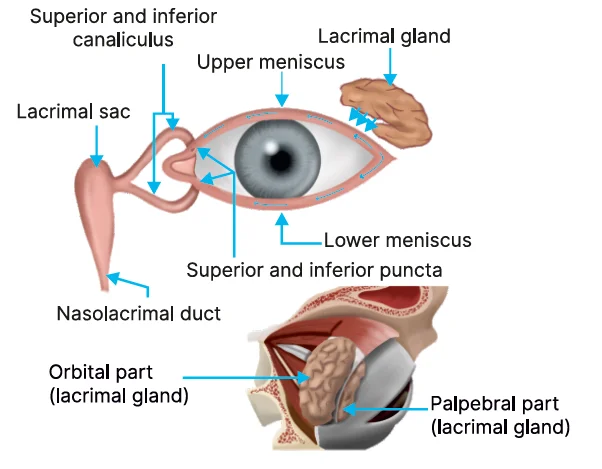
A tear that is formed by the lacrimal gland passes to the upper and lower menisci
↓
Then it passes through the inferior and superior puncta
↓
Then, passes to the superior-inferior canaliculus that forms the common canaliculi
↓
Finally, passes through the lacrimal sac and nasolacrimal duct
Q2.2: Nasolacrimal gland opens into?
Answer: Inferior meatus of the nose.
Q2.3: Where is the inferior meatus present?
Answer: Anteriorly.
Q2.4: What is the alignment of the upper and lower puncta?
Answer: The upper puncta is medial to the lower puncta.
Q2.5: What are the types of watering of the eyes?
Answer:
- Watering is of two types:
- Lacrimation: Hypersecretion
- Overflow: Epiphora
- When there is a problem in the drainage system, it will either cause epiphora or discharge.
- Because of stagnancy, there will be a discharge of water in the eyes.
Q2.6: How is the Regurgitation test used to evaluate lacrimal drainage?
Answer: In the Regurgitation test, the medial canthus of the eye is pressed to determine whether there is any regurgitation, which is an indication of blockage.
Q2.7: What is the slit lamp finding seen in the overflow of the eyes?
Answer: On the slit lamp examination in a patient presenting with watery eyes, if the meniscus height is too high, it indicates there is an overflow, and the problem is in the drainage.
.jpg)
Corneal Stromal Dystrophies
Big Question 3: What are the types, features, and associations of corneal stromal dystrophies?
Broad Answer: Corneal stromal dystrophies are a group of rare, inherited eye disorders that cause abnormal protein or other material to build up in the cornea's middle layer, the stroma. This buildup can lead to a gradual loss of vision due to clouding of the cornea, and the specific type of dystrophy determines the unique pattern and composition of these deposits.
Detailed Questions
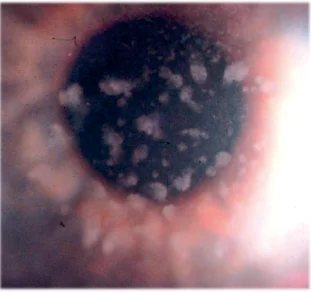
Q3.1: What are the features of macular dystrophy?
Answer:
- Between the lesions, the cornea is hazy
- Colloidal irinol calcium blue is used for Macular dystrophy
- The least common macular dystrophy
- Autosomal recessive (All other are Autosomal dominant)
- It is associated with Mucopolysaccharidosis.
Q3.2: What are the features of granular dystrophy?
Answer:
- Between the lesions, the cornea is clear
- Mason Trichome stain is used for Granular dystrophy
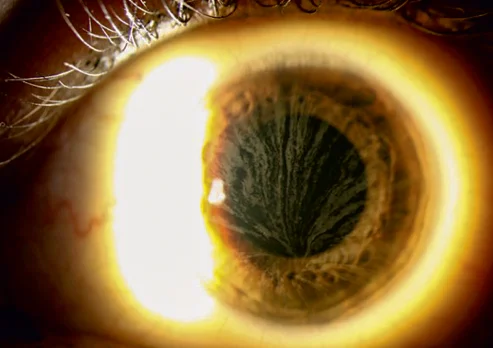
Q3.3: What are the salient features of lattice dystrophy?
Answer:
- Between the lesions, lattice strands are seen
- The most common stromal dystrophy is lattice type 1
- Type 2 lattice is associated with Amyloidosis
- Congo red stain is used for Lattice dystrophy
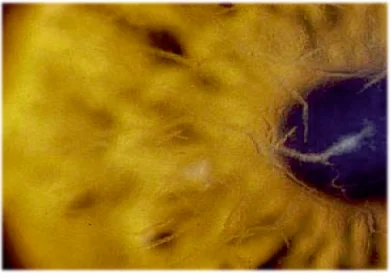
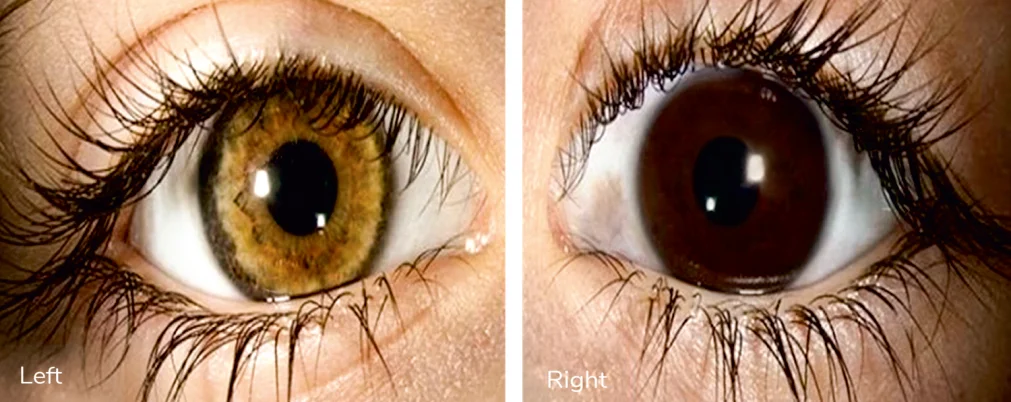
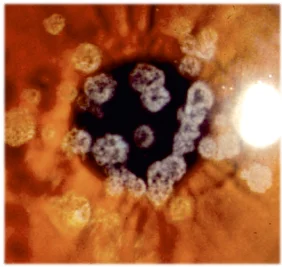
Q3.4: What are Dennie-Morgan folds, and in which conditions are they seen?
Answer:
- The arrows show the folds that are formed due to intense rubbing.
- It is seen in Vernal keratoconjunctivitis/Atopic dermatitis, and allergies.

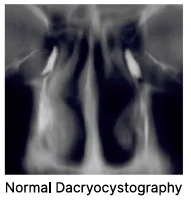
Q3.5: What is dacryocystography, and what structures does it visualise?
Answer: A dye is put, and radiography is taken. Lower and upper canaliculi, sac, and the nasolacrimal duct are seen.
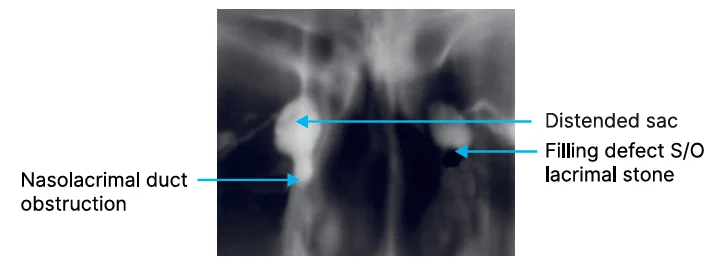
Q3.6: What are the radiological findings of mucocele and dacryolithiasis on dacryocystography?
Answer:
- A mucocele is seen, and a block in the nasolacrimal duct is seen.
- A filling defect is seen on the other side, which shows a Lacrimal stone.
Big Question 4: What are the effects and key features of lesions at different levels of the visual pathway?
Broad Answer: Lesions in the visual pathway cause specific types of visual field defects depending on their location, from the optic nerve to the visual cortex. Each lesion has characteristic field defects such as hemianopia, quadrantanopia, or keyhole vision. The lateral geniculate body is organized into different cellular layers responsible for visual processing. Vascular or traumatic lesions at different points lead to distinct clinical signs, including macular sparing or Optokinetic Nystagmus abnormalities.
Lesions
Detailed Questions
Q4.1: What are the various lesions of the visual pathway?
Answer:
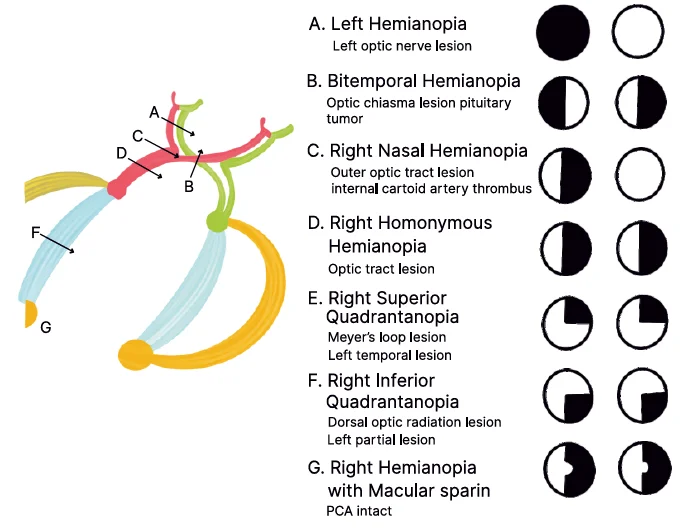
- A: indicates a lesion in the optic nerve: Left Hemianopia.
- B: indicates a lesion in the chiasma: Bitemporal Hemianopia.
- C: indicates a lesion at the junction of chiasma.
- D: indicates a lesion at the optic tract: Right-sided homonymous hemianopia.
- E: indicates a lesion at the temporal radiation fibre: Pie in the sky.
- F: indicates a lesion at the parietal radiation fibre: Pie in floor.
- G: indicates a lesion at the visual cortex: Congruous homonymous hemianopia (shows Macula sparing → Key-hole vision)
Note: In keyhole vision, the lateral geniculate body is seen.
Q4.2: What are the key features of lesions near the junction of the chiasma?
Answer:
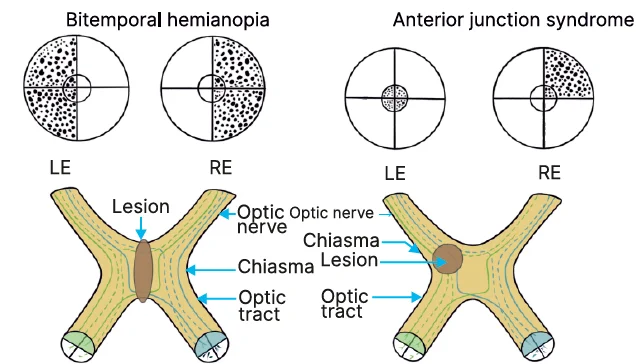
- In the Junctional scotoma at the junction of the chiasma, some part of the nerve has gone.
- If the lesion is at the back, the inferonasal nerve fibres are involved, called Willebrand's knee.
- If inferonasal fibers are involved, a superior temporal field effect is seen due to Willebrand's effect.
- Macular heteronymous hemianopia or posterior junction syndrome is a visual field defect in which vision in either the left or right half of both eyes is absent due to a lesion in the optic chiasm.
Q4.3: What are the features of the Lateral Geniculate Body (LGB) lesions?
Answer:
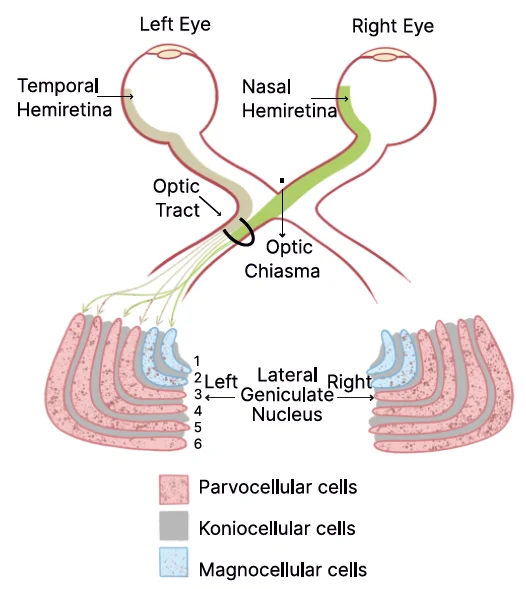
- 1 and 2 in blue color represent magnocellular cells, and 3 to 6 represent parvocellular cells (responsible for colour vision).
- Magnocellular cells consist of larger cells that are responsible for gross movement and motion.
- Koniocellular cells (lamellae) are located in the koniocellular layer of the lateral geniculate nucleus (LGN) (greyish colour), responsible for the blue colour.
Q4.4: Which cells are responsible for colour vision?
Answer: Parvocellular cells.
Q4.5: 1,4,6 and 2,3,5 layers are responsible for which supply?
Answer: Layers 1, 4, and 6 (opposite side-nasal fibers) are in charge of the contralateral eye, while Layers 2, 3, and 5 (same side-temporal fibres) are in charge of the ipsilateral eye.
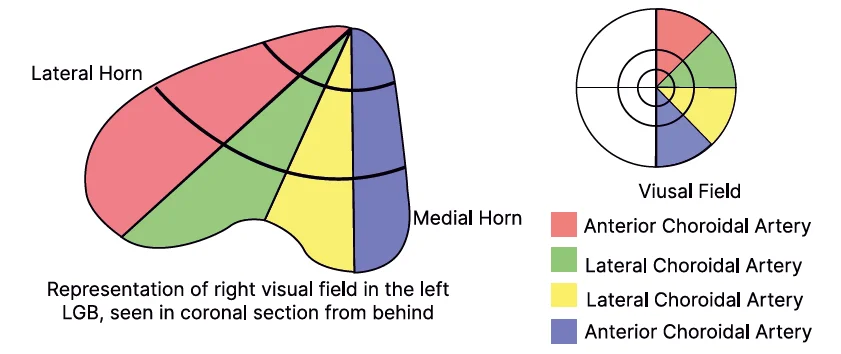
Q4.6: Where is the keyhole visual defect seen?
Answer: LGB lesion.
Q4.7: Which vessel is involved in the keyhole visual defect?
Answer:
Surgical and Diagnostic Techniques
Big Question 5: What are the important surgical and diagnostic techniques used in ophthalmology?
Broad Answer: Various methods are employed in ophthalmology to aid in surgery, lens implantation, and diagnosis. These techniques help improve outcomes and provide better visualisation and correction.
Detailed Questions
Q5.1: Differentiate between Hydrodissection and Hydrodelineation.
Answer:
| Hydrodissection | Hydrodelineation |
| ● We inject between the capsule and the cortex. ● The capsule is separated from the lens | ● The water is between the nucleus, epinucleus, cortex ● The layers are being separated |
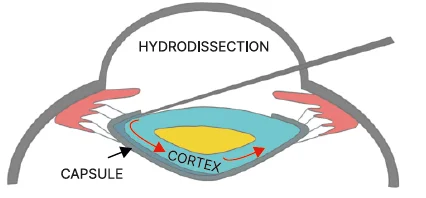
Hydrodissection
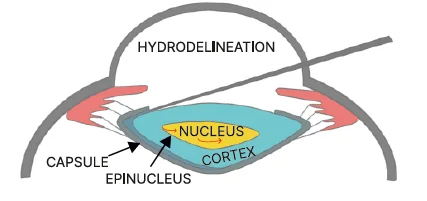
Hydrodelineation
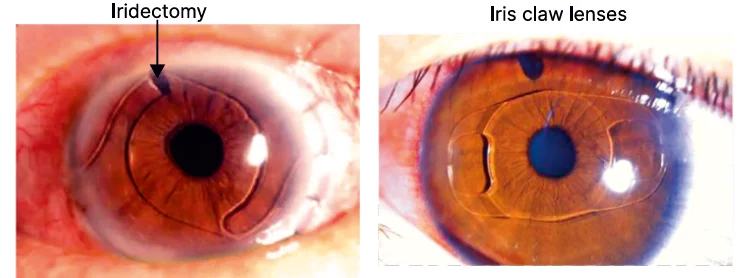
Q5.2: What is the role of iridectomy in lens implantations?
Answer: Iridectomy is required in AC-IOL and iris claw lenses to facilitate proper aqueous drainage.
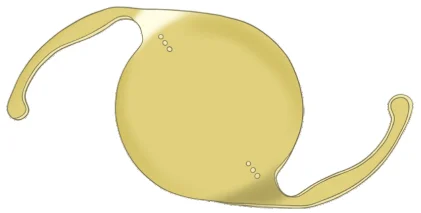
Q5.3: What are the features of multifocal lenses and toric lenses?
Answer:
These are Multifocal lens. It takes care of near, intermediate and far vision.

These are Toric lenses for cylindrical correction.
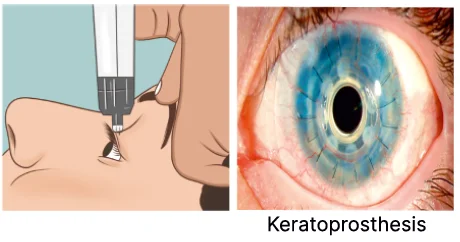
Q5.4: What is a transpalpebral tonometer, and what are its clinical applications?
Answer:
- Transpalpebral tonometer (like digital tonometry)
- It is also known as Diaton.
- It is useful for patients with a Keratoprosthesis.
Q5.5: What are the uses of ultrasound biomicroscopy?
Answer:
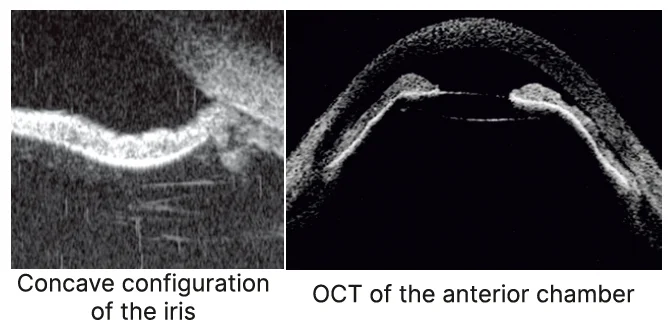
First image: It shows that the configuration of the Iris is concave
- This is pigmentary glaucoma
- This is also called reverse glaucoma
Second image: Anterior segment OCT
- It shows a very shallow anterior chamber
- This is aqueous misdirection syndrome/malignant glaucoma
Anterior-Uveitis
Big Question 6: What is Anterior-Uveitis? Discuss clinical presentation and treatment of choice?
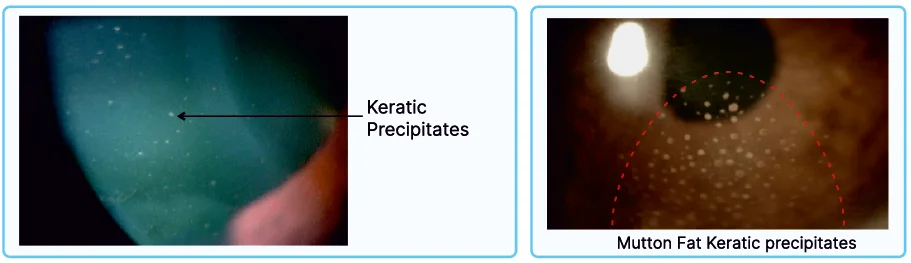
Broad answer: Uveitis is an inflammation of the uveal tissue. Non-granulomatous will be associated with fine Keratic precipitates (these are the deposits at the back/lower of the cornea). KPs are mostly present in the lower cornea due to convection current in aqueous humor. In granulomatous, mutton fat keratic precipitates (KPs) are seen, and found maximum in the imaginary triangular area of eyes called Arlt's triangle.
Detailed Questions
Q6.1. Why are keratin proteins always present at the lower cornea?
Ans. Due to the convection current of aqueous humour.
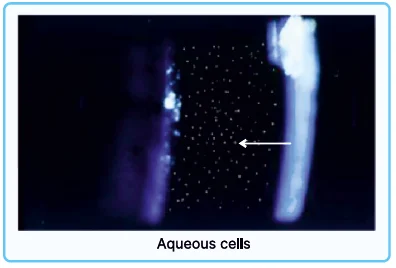
Aqueous Cells
- Sign of active inflammation.
- These cells can come to the iris, and the pupil is always miotic, called a muddy iris.
- In non-granulomatous, Koeppe nodules can be seen.
- In granulomatous, Bussaca nodules can be seen.
- If it adheres to the lens, its called posterior synechiae
- If these cells cover all around the aqueous humour, its called ring synechia.
- This ring synechiae prevents the flow of aqueous humour into the anterior chamber.
- If aqueous collects here, it moves the iris forward and then adheres to the cornea leading to peripheral anterior synechiae (PAS).
- PAS causes angle-closure glaucoma.
- When everything fills, it is called occlusion pupil.
Q6.2. What are the signs of active inflammation?
Ans. Aqueous cells.
Q6.3. The point where these aqueous cells adhere or not move?
Ans. Festoon shape pupil.
Q6.4. What is the treatment of choice for anterior uveitis?
Ans. Topical steroids and Topical cycloplegic.
Topical cycloplegic relaxes the muscles by relieving the ciliary spasm and prevents posterior synechiae.
Q6.5 . What is the Luminate program?
Ans. The Luminate program assesses the safety and efficacy of voclosporin for the treatment of all forms of uveitis.
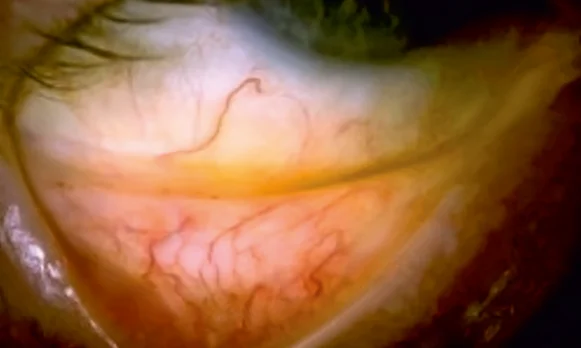
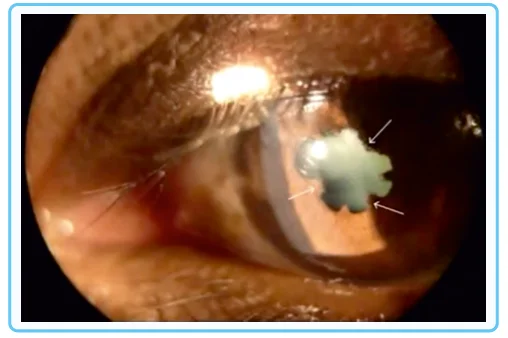
Q6.6 . Identify the picture?
Ans. Iris Bombe
Leads to angle closure.
Also Read : Ophthalmology Image-based Questions for NEET PG Preparation
If you’re looking to strengthen your final prep, don’t miss out on Rapid Revision Reignite by PrepLadder. It’s designed to help Medical PG aspirants cover the entire syllabus quickly with concise notes in a Question-Answer format, high-yield MCQs, and expert-led revision videos—perfect for last-minute reinforcement before the exam.
Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Smarter Video Lectures also in हिंglish, Game Changing Qbank, Audio QBank, Structured Notes, Treasures, Mock test for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Glaucoma
Detailed Questions
Lacrimal Drainage System
Detailed Questions
Corneal Stromal Dystrophies
Detailed Questions
Lesions
Detailed Questions
Surgical and Diagnostic Techniques
Detailed Questions
Anterior-Uveitis
Detailed Questions
Top searching words
The most popular search terms used by aspirants
- NEET PG Ophthalmology Preparation
- NEET PG Ophthamology
- NEET PG Preparation
- Rapid Revision