Nephron Structure: An explanation of the counter-current mechanism
Dec 19, 2025
Despite fluid restriction, a 45-year-old woman with poorly managed diabetes exhibits polyuria, producing almost 4 liters of urine every day. At 180 mOsm/kg, her urine osmolality is still obstinately low. A concentrating defect is suspected by the nephrologist. It is necessary to follow the filtrate's path from the glomerulus to the collecting duct in the nephron in order to comprehend why she is unable to concentrate urine. Everything from blood pressure to acid-base balance is determined by this single functional unit, which is duplicated a million times per kidney. This is rigorously tested by NEET PG.
QUICK ANSWER
The glomerulus (filtration), proximal convoluted tubule (bulk reabsorption), loop of Henle (concentration gradient creation), distal convoluted tubule (fine-tuning), and collecting duct (final concentration) make up the nephron, the kidney's functional unit. Urine concentrations up to 1200 mOsm/kg are made possible by the counter-current mechanism, which creates a medullary osmotic gradient (300-1200 mOsm/L) via the counter-current multiplier (loop of Henle) and counter-current exchanger (vasa recta).
NEET PG RELEVANCE
Every year, six to ten questions on NEET PG papers deal with nephron physiology. The ADH mechanism, PCT vs. DCT transport differences, site-specific actions of diuretics, and the counter-current multiplier mechanism are among the focus areas. Aquaporin channels, tubuloglomerular feedback, and clinical associations with concentrating defects are highlighted in recent studies.

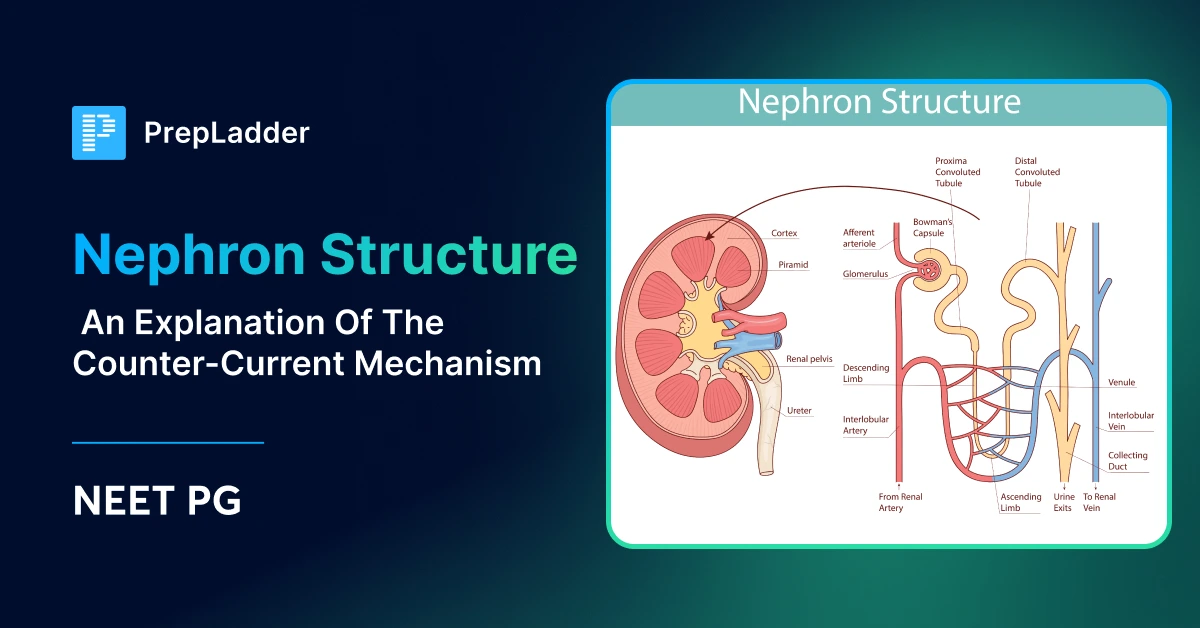
A Nephron: What is it?
The kidney's structural and functional unit is the nephron. About 1 million nephrons make up each human kidney, which filters 180 litres of plasma every day while only producing 1-2 litres of urine.
Consider the nephron as an advanced recycling facility. With the exception of proteins and cells, almost everything can pass through the glomerulus, which functions as an indiscriminate filter. 99% of this filtrate is then selectively recovered by the tubular system, retaining what the body requires while eliminating waste into urine.
Based on location, there are two types of nephrons. Eighty-five percent of cortical nephrons have short Henle loops that hardly penetrate the medulla. In order to produce the concentrated medullary interstitium needed for water conservation, juxtamedullary nephrons (15%) have long loops that extend deep into the inner medulla.
Afferent arterioles supply blood to the nephron by feeding glomerular capillaries, which subsequently reform as efferent arterioles. These efferent vessels develop into peritubular capillaries that surround cortical nephrons or vasa recta in conjunction with juxtamedullary nephron loops. This particular portal arrangement is unique to the body.
What Constitutes a Nephron?
Each segment of the nephron uses specific cell types and transport systems to carry out unique tasks. Clinical syndromes are explained and diuretic actions are predicted by an understanding of segmental physiology.
Corpuscle of the Renal
The glomerular capillary tuft is surrounded by Bowman's capsule, which makes up the renal corpuscle. The glomerular basement membrane (GBM), podocyte foot processes with slit diaphragms, and fenestrated endothelium are the three filtration barriers that keep blood and filtrate apart.
This barrier freely filters substances with molecular weights less than 7 kDa. Albuminuria is a sensitive indicator of glomerular damage because albumin (69 kDa) is largely retained. Anionic proteins are also repelled by the GBM's negative charge; the loss of this charge barrier explains nephrotic-range proteinuria in minimal change disease.
A normal GFR is 180 L/day, or 125 mL/min. One-fifth of the plasma passing through glomeruli becomes filtrate when the filtration fraction (GFR/RPF) is typically 20%.
|
|
|
|
|
|
|
|
|
|
|
|
PCT, or proximal convoluted tubule
65–70% of filtered sodium, water, bicarbonate, glucose, amino acids, and phosphate are reabsorbed by the PCT. Its brush border membrane greatly expands the transportation surface area.
Here, sodium reabsorption is iso-osmotic, with water following passively to keep tubular fluid osmolality at 300 mOsm/L during the PCT.
This process is driven by the Na+/K+-ATPase on basolateral membranes, which produces gradients that luminal co-transporters take advantage of.
SGLT2 (90%) and SGLT1 (10%) are responsible for glucose reabsorption in early and late PCT, respectively. For glucose, the transport maximum (Tm) is roughly 375 mg/min.
Glycosuria in uncontrolled diabetes is explained by glucosuria, which occurs when plasma glucose levels surpass the renal threshold of 180 mg/dL.
Additionally, PCT secretes organic cations (creatinine, medications like cimetidine) and organic anions (uric acid, medications like penicillin).
Drug interactions are explained by this secretory function, which also serves as the foundation for PAH clearance measurements of renal plasma flow.
Henle's Loop
The medullary concentration gradient necessary for water conservation is produced by the loop of Henle. The counter-current multiplier mechanism is made possible by its hairpin configuration.
The thin descending limb is impermeable to solutes but extremely permeable to water. Water passively leaves the filtrate as it descends into the increasingly hypertonic medulla, concentrating tubular fluid to 1200 mOsm/L at the hairpin turn.
Water cannot pass through the thick ascending limb (TAL), but the Na+-K+-2Cl-cotransporter (NKCC2) actively moves sodium, potassium, and chloride. The medullary gradient is produced by multiplying this "single effect" of about 200 mOsm/L difference along the loop's length. Because the filtrate exiting TAL is hypotonic (100 mOsm/L), it is referred to as the "diluting segment."
The concentrating gradient is eliminated, and copious amounts of diluted urine are produced when loop diuretics (furosemide, bumetanide) inhibit NKCC2.
DCT, or distal convoluted tubule
Through the thiazide-sensitive Na+-Cl-cotransporter (NCC), the DCT keeps diluting the filtrate. Regardless of ADH status, DCT is impermeable to water, in contrast to PCT.
Calcium reabsorption here is regulated by PTH, which stimulates apical calcium channels (TRPV5) and basolateral Ca2+-ATPase. Thiazide diuretics paradoxically increase calcium reabsorption—explaining their use in hypercalciuria and nephrolithiasis prevention.
The macula densa, a specialized sensor that measures tubular sodium chloride concentration, is another component of the DCT. The macula densa initiates tubuloglomerular feedback when NaCl delivery rises (indicating volume overload), narrowing afferent arterioles to lower GFR and releasing renin to restore volume.
Also Read: How to Read an ECG: Waves, Intervals, Axis Deviation
Collecting Duct
The collecting duct makes the final decision on urine concentration through principal cells and intercalated cells.
Principal cells respond to aldosterone (sodium reabsorption via ENaC, potassium secretion) and ADH (water reabsorption via aquaporin-2 insertion). Intercalated cells regulate acid-base balance—type A cells secrete H+ in acidosis, while type B cells secrete HCO3- in alkalosis.
ADH (vasopressin) binds V2 receptors on principal cells, triggering cAMP-mediated insertion of aquaporin-2 channels into apical membranes. This makes collecting ducts permeable to water, allowing equilibration with hypertonic medullary interstitium and producing concentrated urine up to 1200 mOsm/kg.
How Does the Counter-Current Mechanism Work?
The counter-current mechanism maintains medullary hypertonicity through two complementary systems: the counter-current multiplier in the loop of Henle and the counter-current exchanger in vasa recta.
Multiplier with Counter-Current
A small transverse gradient is amplified into a large longitudinal gradient by this mechanism. The process starts with a single effect: TAL pumps NaCl into the interstitium, causing the tubular fluid and surrounding medulla to differ by 200 mOsm/L.
This one effect multiplies along the length of the loop because ascending and descending limbs run parallel with the flow in opposing directions. Filtrate is concentrated as water exits the descending limb, giving the ascending limb more solute to pump out.
The corticomedullary junction has 300 mOsm/L of medullary osmolality at steady state, while the papillary tip has 1200 mOsm/L. This gradient is always present; ADH just needs to take advantage of it to conserve water.
About half of the inner medullary osmolality comes from urea. Through UT-A1 transporters, ADH increases urea permeability in inner medullary collecting ducts, enabling urea recycling into the interstitium. Maximum urine concentration depends on this urea recycling; patients with protein malnutrition are unable to do so because of inadequate urea.
Also Read: Rapid Revision Reignite Physiology: Question-Answer Format
Counter-Current Exchanger
The vasa recta preserve the medullary gradient that the loop of Henle creates. These vessels run parallel to loops of Henle with sluggish, counter-current blood flow.
Blood equilibrates with the surrounding hypertonic interstitium as it descends into the medulla, losing water and gaining solutes. The process reverses as it rises, with water returning to the blood and solutes returning to the interstitium. While providing oxygen to medullary structures, this passive exchange stops medullary washout.
Concentration is hampered by increased medullary blood flow (as in volume expansion), which washes out the gradient. This explains why conditions that increase renal blood flow result in diluted urine.
| A feature | Multiplier with Counter-Current | Counter-Current Exchanger |
| Organization | Henle's Loop | Vasa Recta |
| Procedure | Passive (TDL) + Active (TAL) | Completely Passive |
| Function | produces a medullary gradient | maintains the medullary gradient |
| Important Carrier | None (just diffusion) | |
| Energy Needed | ATP-regulated | No ATP required |
| The Impact of Disruption | loss of ability to focus | Medullary washout |
How is Urine Concentration Regulated?
ADH-mediated water permeability in collecting ducts and an intact medullary gradient are the two factors that determine urine concentration.
ADH's (vasopressin) function
The hypothalamic supraoptic and paraventricular nuclei produce ADH, which is then stored in the posterior pituitary and released in response to either decreased blood volume (which is detected by baroreceptors) or increased plasma osmolality (which is detected by osmoreceptors).
Adenylyl cyclase is activated, and cAMP is increased when ADH binds to V2 receptors on collecting duct principal cells. Protein kinase A is activated as a result, phosphorylating aquaporin-2 (AQP2) storage vesicles and causing them to fuse with apical membranes. After entering cells through AQP2, water leaves through constitutive AQP3 and AQP4 on basolateral membranes.
Maximum ADH effect produces urine osmolality of 1200 mOsm/kg (specific gravity ~1.035). ADH absence produces dilute urine of 50-100 mOsm/kg (specific gravity ~1.001).
Also Read: Last 5-Year PYQs in Physiology for INI-CET
Clinical Associations
Concentrating defects are seen in diabetes insipidus (DI). Nephrogenic DI is caused by collecting duct resistance to ADH, whereas central DI is caused by insufficient ADH secretion. They can be distinguished by the water deprivation test; nephrogenic DI does not react to exogenous desmopressin, whereas central DI does.
Despite low plasma osmolality, SIADH (syndrome of inappropriate ADH) causes concentrated urine. Urine osmolality >100 mOsm/kg with plasma osmolality <275 mOsm/kg, euvolemic state, and urine sodium >40 mEq/L are diagnostic criteria.
A common NEET PG question is that lithium causes nephrogenic DI by downregulating the expression of AQP2. Both hypokalemia and hypercalcemia make it difficult to focus.
| A feature | P-C | The DCT | Collecting Duct |
| % Reabsorbed Na+ | 65–70% | 5–8% | 2–5% |
| Permeability of Water | Permeable at all times | Impermeable at all times | ADH-related |
| Important Carrier | SGLT2 and Na+/K+-ATPase | NCC (sensitive to thiazides) | AQP2 and ENaC |
| Regulation of Hormones | II angiotensin | For Ca2+, PTH | ADH and aldosterone |
| Here, a diuretic is acting | Inhibitors of carbonic anhydrase | Thiazoles | Diuretics that spare K+ |

High-Yield Points for NEET PG
- Each kidney has about one million nephrons; GFR is 125 mL/min, or 180 L/day.
- 65–70% of filtered Na+, water, glucose, bicarbonate, amino acids, and phosphate are reabsorbed by PCT in an iso-osmotically
- Renal threshold = 180 mg/dL; glucose Tm = 375 mg/min; SGLT2 inhibitors (dapagliflozin) induce deliberate glucosuria
- The "diluting segment" is TAL, which is impermeable to water and actively pumps NaCl via NKCC2. Loop diuretics work here.
- Medullary gradient: 300–1200 mOsm/L; urea recycling accounts for 50% of this.
- V2 receptors are affected by ADH, which leads to cAMP, AQP2 insertion, and water reabsorption.
- Urine concentration ranges from 50 mOsm/kg (without ADH) to 1200 mOsm/kg (with ADH).
- The gradient is produced by the counter-current multiplier (loop) and maintained by the counter-current exchanger (vasa recta).
- When the macula densa detects the delivery of NaCl, tubuloglomerular feedback and renin release are triggered.
- Nephrogenic DI is brought on by lithium, hypercalcemia, and hypokalemia, all of which impair concentration.
"Please Cook Delicious Tacos Constantly" is a nephron segment mnemonic that includes PCT, Cortical TAL, DCT, Thick Medullary Collecting Duct, and Collecting Duct.
Mnemonic for diuretic sites: "CAP The Losers" — Carbonic anhydrase inhibitors (PCT), Aldosterone antagonists (CD), Potassium-sparing (CD), Thiazides (DCT), Loop diuretics (TAL)
Also Read: Insulin Receptors: Structure, Functions and Action
Frequently Asked Questions
What distinguishes an exchanger from a counter-current multiplier?
The counter-current multiplier (loop of Henle) actively creates the medullary osmotic gradient through ATP-dependent NaCl transport in the thick ascending limb. The counter-current exchanger (vasa recta) passively preserves this gradient through equilibration without energy expenditure. Multiplier generates; exchanger maintains.
Why is the thick ascending limb called the diluting segment?
The thick ascending limb is impermeable to water but actively pumps NaCl into the interstitium through the NKCC2 cotransporter. By separating the solute from the water, tubular fluid is diluted to about 100 mOsm/L as it exits, which is much less than plasma's 300 mOsm/L. This diluting ability is eliminated by loop diuretics.
How is urine concentrated by ADH?
ADH increases intracellular cAMP by binding to V2 receptors on collecting duct principal cells. Collecting ducts become water-permeable as a result of the insertion of aquaporin-2 (AQP2) channels into apical membranes. Urine is then concentrated up to 1200 mOsm/kg as water passes passively down its concentration gradient into the hypertonic medullary interstitium.
Nephrogenic diabetes insipidus: what causes it?
Despite sufficient hormone levels, collecting duct resistance to ADH causes nephrogenic DI. The most frequent medication causes, such as lithium therapy, hypercalcemia, hypokalemia, chronic kidney disease, and genetic mutations in the V2 receptor or AQP2 genes, are among the causes. Large amounts of diluted urine are produced by patients who do not respond to desmopressin.
Why is urine concentration affected by protein malnutrition?
About half of the inner medullary osmolality comes from urea. Hepatic urea synthesis declines in protein malnutrition, which lowers the osmotic gradient and medullary urea content.
The reduced gradient restricts the maximum urine concentration, usually to 600–800 mOsm/kg, even with normal ADH secretion and collecting duct function.
Which area of the kidney do thiazide diuretics target?
Thiazides prevent about 5-8% of sodium reabsorption by inhibiting the Na+-Cl-cotransporter (NCC) in the distal convoluted tubule. Thiazides are helpful for hypercalciuric nephrolithiasis because, in contrast to loop diuretics, they improve calcium reabsorption in DCT. Their comparatively mild natriuretic effect is ideal for managing chronic hypertension.
CLINICAL PEARL
"The kidney protects the internal environment in addition to producing urine." Examine the concentrating mechanism methodically when a patient exhibits polyuria: Check urea and medullary blood flow to see if the medullary gradient is still intact. Does ADH (plasma osmolality, ADH levels) exist? Is the collecting duct reacting to the challenge of desmopressin?
Every clinical syndrome has elegant physiology, as the nephron teaches us, and NEET PG rewards those who comprehend the mechanism rather than merely memorize the associations.
Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Video Lecturesalso in हिंglish, digital notes, QBank, and Mock Tests for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
A Nephron: What is it?
What Constitutes a Nephron?
Corpuscle of the Renal
PCT, or proximal convoluted tubule
Henle's Loop
DCT, or distal convoluted tubule
Collecting Duct
How Does the Counter-Current Mechanism Work?
Multiplier with Counter-Current
Counter-Current Exchanger
How is Urine Concentration Regulated?
ADH's (vasopressin) function
Clinical Associations
High-Yield Points for NEET PG
Frequently Asked Questions
Which area of the kidney do thiazide diuretics target?
CLINICAL PEARL
Top searching words
The most popular search terms used by aspirants
- Medical PG Preparation
- NEET PG Exam Preparation
- NEET PG Physiology Preparation
- NEET PG Preparation Strategy