High-Yield Dermatology for NEET PG 2026: Skin Conditions & MCQ Pearls
Apr 20, 2026
The Case That Changes Everything
A 35-year-old farm worker presents with multiple flaccid blisters that extend across his torso and mouth. The lesions become radioactive when they break because they create extremely painful open wounds. The test for Nikolsky sign shows a positive result. The direct immunofluorescence test shows an intercellular pattern that resembles a fishnet design of IgG that binds to skin proteins, while serum testing shows elevated levels of anti-desmoglein 3 antibodies. The diagnosis of pemphigus vulgaris occurs when the condition affects the epidermal layer, which exists above the basal layer.
The NEET PG examination tests candidates through this clinical case study, which represents a standard test question about pemphigus vulgaris. The dermatology section of the exam contains 8 to 12 questions, which focus on particular disease patterns, allowing students to gain 15 to 20 marks through complete topic knowledge.
QUICK ANSWER
The essential dermatological material for NEET PG candidates includes vesiculobullous disorders, papulosquamous diseases, leprosy classification, drug-induced reactions, and pigmentary abnormalities. The five most commonly examined medical conditions include pemphigus vulgaris, psoriasis, leprosy (Hansen’s disease), Stevens-Johnson syndrome (SJS), and lichen planus.
The primary treatment for pemphigus vulgaris consists of administering systemic corticosteroids in the form of prednisolone at a dosage of 1-2 mg per kilogram of body weight. Direct immunofluorescence (DIF) remains the definitive diagnostic method for all bullous skin disorders.
NEET PG RELEVANCE
NEET PG examinations use dermatology as a major subject, which generates 8-12 questions for each testing session. The essential knowledge areas include vesiculobullous disorders, which compare pemphigus with pemphigoid, the WHO multidrug therapy (MDT) system for leprosy, and psoriasis treatment methods, plus the analysis of drug-related skin reactions that result in SJS/TEN. Recent exams have shown that students now need to understand how to interpret immunofluorescence patterns and dermoscopic diagnostic elements.
Here’s an outline covering essential dermatology areas relevant to NEET PG preparation:
- Vesiculobullous Disorders: Pemphigus versus Pemphigoid
- Psoriasis: Pathogenesis, Variants, and Therapeutic Hierarchy
- Leprosy: Ridley-Jopling Classification and WHO-MDT Guidelines
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis
- Lichen Planus: Clinical Features (“6 Ps”) and Subtypes
- Pigmentary Disorders: Vitiligo and Melasma
- The Comparative Summary Table outlines information about six major dermatologic diseases
- High-Yield Points for NEET PG
- The document provides answers to frequently asked questions.

Why Dermatology Is a Scoring Gold Mine in NEET PG
In the NEET PG exam, dermatology offers a strong scoring advantage because of its exceptional value to students. Dermatology provides NEET PG students with multiple benefits because the subject has clear boundaries, and students can expect to see similar questions throughout their studies.
The academic research conducted over several decades shows that 15 to 20 main medical conditions repeat themselves in every examination cycle with consistent frequency. The success of this field requires professionals to identify patterns in both clinical situations and examination tests because they need to distinguish between two similar clinical situations to achieve correct assessment results.
Vesiculobullous Disorders - Pemphigus vs Pemphigoid
Among all dermatological topics for NEET PG study, this area stands out as the highest-yield section due to its clear comparative parameters.
Pemphigus Vulgaris:
- The condition exists as an autoimmune disorder that causes blistering through IgG autoantibodies to desmoglein 3 and desmoglein 1, which leads to epidermal cell junction loss through acantholysis.
- The lesions present as soft blisters that lose their structure upon contact with any object.
- The first signs of the disease appear on the oral mucosa before they develop into skin symptoms.
- The test shows a positive result for the Nikolsky sign.
- The histopathological study demonstrates suprabasal acantholysis, which creates the "row of tombstones" appearance because basal cells remain connected to the basement membrane zone.
- The direct immunofluorescence test shows intercellular IgG and C3 deposits in a typical fishnet pattern.
- The management plan uses systemic corticosteroids as the primary treatment method, while doctors can prescribe azathioprine, mycophenolate mofetil or rituximab as supplementary treatments for extended patient care.
- The RITUX 3 trial, which was published in The Lancet (2017), demonstrates that rituximab delivers better treatment results than standard immunosuppressive drugs. The image shows direct immunofluorescence results through the application of an anti-IgG antibody.
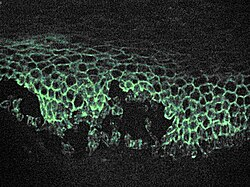
Microscopic image of direct immunofluorescence using an anti-IgG antibody.
Bullous Pemphigoid
- Bullous Pemphigoid is the most prevalent autoimmune blistering disorder among individuals older than sixty years.
- Autoantibodies target BP antigen 180 (BPAg2) and BP antigen 230 (BPAg1) located at the dermoepidermal junction.
- Bullae in this condition show different clinical features from pemphigus vulgaris because they present with tense bullae and a negative Nikolsky sign, which makes oral involvement rare, but patients experience pruritus before developing lesions.
- The histopathology examination shows subepidermal blistering that occurs with eosinophilic infiltration.
- The basement membrane zone shows linear IgG/C3 deposition, which serves as a differential diagnostic test because it shows a different pattern from the intercellular "fishnet" pattern found in pemphigus vulgaris.
- The direct immunofluorescence study shows linear immunoglobulin G and C3 deposits that extend along the dermoepidermal junction.
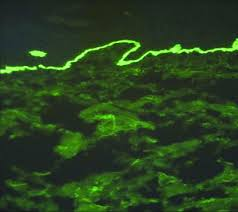
Direct immunofluorescence study showing linear immunoglobulin G and C3 deposits along the dermoepidermal junction
The ability to identify these differences permits dermatologists to make accurate diagnoses, which are necessary for their medical work and their NEET PG dermatology preparation.
Also Read: Modes of Ventilation: Types and Uses
Psoriasis - Pathogenesis, Types & Treatment Ladder
Psoriasis is a long-term skin condition that develops through an immune response to T cells, which creates papulosquamous symptoms that produce distinct red patches with silvery-white scales. The condition affects around 2 to 3 per cent of people worldwide.

Pathogenesis:
- Th17 cells release interleukins IL-17 and IL-22, which cause keratinocytes to multiply at an accelerated rate.
- The epidermis experiences an accelerated turnover process, which decreases its normal 28-day cycle to a 3-to-4-day period.
- The primary cytokines that drive this process include TNF-α, IL-23 and IL-17A, which researchers use as clinical targets for biological therapies.
- The histopathological examination shows parakeratosis and regular acanthosis and Munro microabscesses that contain neutrophilic aggregates inside the stratum corneum, while the dermal papillae contain dilated tortuous capillaries.
- The Auspitz sign appears when pinpoint bleeding happens after scale removal.
- Microscopic observation shows hypogranulosis and an influx of numerous neutrophils in the corneal layer.
hypogranulosis, and an influx of numerous neutrophils in the corneal layer
Clinical Variants:
- Chronic plaque psoriasis (psoriasis vulgaris) constitutes approximately 90% of cases and predominantly affects extensor surfaces, the scalp, and the sacral region.
- Guttate psoriasis presents as small drop-like lesions, which often develop after streptococcal pharyngitis, while children with the condition commonly display elevated antistreptolysin O (ASO) titres.
- Pustular psoriasis features sterile pustules, while its generalised form (von Zumbusch type) constitutes a medical emergency.
- Erythrodermic psoriasis involves more than 90% of the body surface area and poses a life-threatening condition.
- Psoriatic arthritis affects 20 to 30 per cent of people with psoriasis, who show specific "pencil-in-cup" bone deformities on X-ray imaging and experience dactylitis, which causes their fingers to resemble sausages.
Treatment Algorithm:
- Mild disease affecting less than 10 per cent of body surface area is treated with emollients together with topical corticosteroids and vitamin D analogues that include calcipotriol.
- The second stage of treatment starts when either a patient develops moderate disease, which affects 10 to 20 per cent of their body surface area or when previous treatments fail.
- The primary treatment of phototherapy uses NB-UVB at 311 nm, while PUVA serves as the secondary option for patients with resistant conditions.
- The first-line treatment for severe and refractory cases uses systemic agents, which include methotrexate as the primary treatment and cyclosporine and acitretin as additional options.
- The fourth step of treatment begins with patients who meet requirements for biologic medications. The treatment options include TNF-α inhibitors, which consist of etanercept and infliximab, together with IL-17 inhibitors and IL-23 inhibitors, which include secukinumab and guselkumab.
An exam trap notes that Methotrexate contains a pregnancy contraindication, which leads to Category X status, and the drug needs monitoring because it can cause liver damage and bone marrow suppression.
Acitretin works as the primary systemic retinoid treatment for pustular psoriasis. Students often mix up these two medical indications. Our dermatology immunosuppressant guide provides complete information about immunosuppressants used in dermatology.
For a detailed breakdown of immunosuppressants in dermatology, see our guide on Immunosuppressive Drugs for NEET PG.
Leprosy - Ridley-Jopling Classification & WHO-MDT
Leprosy, also known as Hansen disease, is a chronic granulomatous infection that results from the Mycobacterium leprae bacterium, which exists as an obligate intracellular acid-fast bacillus that infects Schwann cells and skin macrophages. India accounts for over 50% of new global leprosy cases annually, which establishes this disease as a popular testing subject for NEET PG examinations.
Also Read: Last 5 Year PYQs in Dermatology for NEET PG
Ridley-Jopling Classification
This spectrum classifies leprosy based on the host's immune response:
| Type | Immune Response | Skin Lesions | Nerve Involvement | Bacillary Load (BI) |
| Tuberculoid (TT) | Strong cell-mediated | Few, well-defined, hypopigmented, anaesthetic | Single nerve, early | Negative (paucibacillary) |
| Borderline Tuberculoid (BT) | Moderate | Few satellite lesions | Few nerves | Low |
| Borderline (BB) | Unstable | "Swiss cheese" / punched-out | Multiple | Moderate |
| Borderline Lepromatous (BL) | Weak | Many bilateral diffuse | Many | High |
| Lepromatous (LL) | Absent/anergy | Diffuse infiltration, leonine facies, madarosis | Glove-and-stocking neuropathy | Very high (multibacillary) |
On the wards, I always teach this using the spectrum analogy: TT is your immune system fighting hard (few bacilli, strong granulomas), while LL is surrender (massive bacillary load, foamy macrophages called Virchow cells/lepra cells).
WHO-MDT Regimen
Paucibacillary (PB): Dapsone (100 mg daily, self-administered) + Rifampicin (600 mg monthly, supervised) - 6 months.
Multibacillary (MB): Dapsone (100 mg daily) + Clofazimine (50 mg daily self-administered, 300 mg monthly supervised) + Rifampicin (600 mg monthly, supervised) - 12 months.
Key side effects to remember:
- Dapsone: haemolytic anaemia (especially in G6PD deficiency), methemoglobinaemia.
- Clofazimine: reddish-brown skin discolouration.
- Rifampicin: hepatotoxicity, red-orange urine.
Lepra Reactions (Exam Favourite)
Type 1 (Reversal Reaction): Cell-mediated, seen in borderline types. Existing lesions become erythematous and oedematous. Treat with systemic corticosteroids.
Type 2 (Erythema Nodosum Leprosum / ENL): Immune complex-mediated, seen in BL/LL. Painful subcutaneous nodules + systemic features (fever, arthralgia). Treat with thalidomide (drug of choice) or corticosteroids. Thalidomide is absolutely contraindicated in pregnancy (teratogenic - recall the phocomelia disaster).
Examiners commonly test the distinction between Type 1 and Type 2 reactions - memorise the mechanism and the treatment.
Stevens-Johnson Syndrome & Toxic Epidermal Necrolysis
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) together represent a severity spectrum of the same drug-induced, immune-mediated mucocutaneous reaction.
SJS involves less than 10% of body surface area detachment, while SJS-TEN overlap covers 10 to 30% of body surface area, and TEN affects more than 30% of body surface area.
The most common causative drugs (mnemonic: "PACE-S" Phenytoin, Allopurinol, Carbamazepine, Antibiotics like sulfonamides, and NSAIDs like piroxicam) should be on the tip of your tongue.
In clinical practice, I have seen carbamazepine and allopurinol as the two most frequent culprits. HLA-B*1502 (carbamazepine-associated SJS in Southeast Asian populations) is a favourite pharmacogenomics question.
Pathology: Keratinocyte apoptosis occurs through Fas-FasL interactivity together with granulysin, which serves as the fundamental biomarker for initial diagnostics. The histological analysis reveals complete epidermal necrosis throughout the entire thickness of the skin.
Treatment:
- The first step in treatment requires doctors to immediately discontinue all drugs that caused the problem.
- The treatment requires patients to receive supportive care inside a burns unit or an intensive care unit.
- Studies have reported IV immunoglobulin (IVIG) and cyclosporine to provide advantages.
- The use of corticosteroids continues to be a topic of disagreement.
- The SCORTEN score predicts mortality; a score ≥ 3 carries > 35% mortality.
Explore drug-induced reactions in depth with Adverse Drug Reactions for NEET PG.
Lichen Planus - The 6 Ps and Variants
Lichen planus is a T-cell-mediated inflammatory dermatosis. The classic presentation is remembered by the 6 Ps: Pruritic, Purple/violaceous, Polygonal, Planar (flat-topped), Papules, and Plaques. Wickham striae — fine white lines on the surface of lesions — are pathognomonic.
Common sites: flexor surfaces of wrists, shins, oral mucosa, genitalia, nails, and scalp.
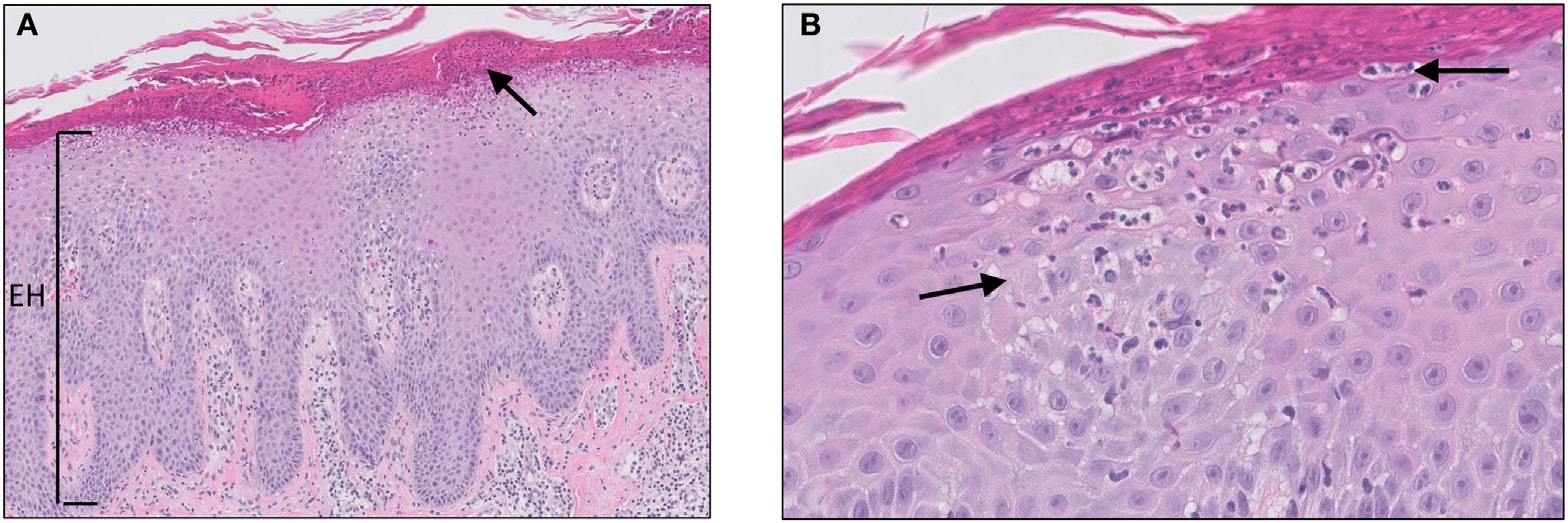
Histopathology: Interface dermatitis with a band-like (lichenoid) lymphocytic infiltrate at the dermoepidermal junction. Civatte bodies (colloid/apoptotic bodies) in the lower epidermis. "Saw-tooth" pattern of irregular acanthosis.
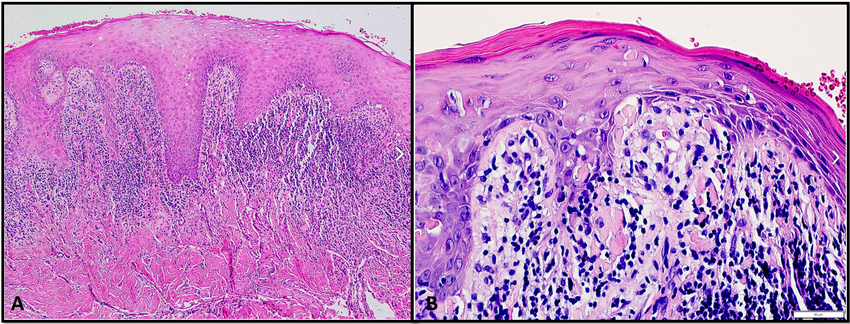
A) Lichen planus shows saw tooth rete ridges and B) Colloid bodies.
Association to remember: Lichen planus + Hepatitis C virus — this link is tested repeatedly. On NEET PG, expect questions linking violaceous polygonal papules on wrists to HCV serology.
Treatment: Potent topical corticosteroids for localised disease. Oral corticosteroids or acitretin for widespread/erosive variants.

Pigmentary Disorders - Vitiligo & Melasma
Vitiligo is an autoimmune disorder causing progressive destruction of melanocytes, resulting in well-defined, depigmented (chalk-white), non-scaly macules and patches. Wood lamp examination enhances lesions (bright white fluorescence). Associations: thyroid disorders (most common), diabetes mellitus, pernicious anaemia, and Addison's disease.

Non-segmental vitiligo of the hand
Treatment: Narrow-band UVB phototherapy is the first-line for generalised vitiligo (>20% BSA). Topical tacrolimus (a calcineurin inhibitor) is preferred for facial lesions, especially in children. For stable, localised vitiligo: melanocyte transfer surgery.
Melasma is an acquired hyperpigmentation disorder, most common in women of reproductive age, exacerbated by UV exposure and hormonal factors (pregnancy, oral contraceptive pills). Distribution: centrofacial (most common), malar, mandibular. Treatment: strict photoprotection + topical triple combination (hydroquinone 2-4% + tretinoin + mild corticosteroid - Kligman formula).

Melasma
Master Comparison Table: Top Dermatology Conditions for NEET PG
Feature Pemphigus Vulgaris Bullous Pemphigoid Psoriasis Leprosy (LL) SJS/TEN Lichen Planus Age group 40-60 years > 60 years Any (peak 20-30) Any Any (drug-dependent) 30-60 years Primary lesion Flaccid blisters/erosions Tense blisters Erythematous scaly plaques Diffuse infiltration, nodules Targetoid lesions, epidermal detachment Violaceous flat-topped papules Key sign Nikolsky +ve Nikolsky -ve Auspitz sign Glove-stocking anaesthesia Nikolsky +ve Wickham striae Histology Suprabasal acantholysis Subepidermal blister Munro microabscesses Virchow cells (lepra cells) Full-thickness epidermal necrosis Saw-tooth acanthosis, Civatte bodies DIF / Key test Fishnet IgG (intercellular) Linear IgG (BMZ) Clinical + biopsy Slit-skin smear, biopsy SCORTEN for prognosis Band-like lymphocytic infiltrate First-line Rx Prednisolone + rituximab Potent topical steroids/doxycycline Topical steroids + calcipotriol WHO-MDT Drug withdrawal + supportive Topical corticosteroids NEET PG pearl Fishnet DIF = PV always Most common autoimmune blistering disease Guttate → Strep throat link Type 1 vs Type 2 reaction HLA-B*1502 + carbamazepine Lichen planus + HCV association
Also Read: Important Topics in Dermatology for NEET-PG
High-Yield Points for NEET PG
- Pemphigus vulgaris: Suprabasal acantholysis + fishnet DIF + anti-desmoglein 3 antibodies. Nikolsky sign is positive.
- Bullous pemphigoid: Subepidermal blister + linear DIF at BMZ + tense blisters in the elderly. It is the most common autoimmune blistering disease.
- Auspitz sign (pinpoint bleeding on scale removal) is pathognomonic for psoriasis. Koebner phenomenon is seen in psoriasis, lichen planus, and vitiligo.
- Guttate psoriasis is triggered by Group A Streptococcal pharyngitis - always link ASO titre elevation with guttate lesions.
- Leprosy: First nerve to be affected = posterior tibial nerve. Most commonly affected nerve = ulnar nerve. Only nerve palpable in the cubital fossa = ulnar nerve.
- Mnemonic for MDT drugs - "R-D-C": Rifampicin, Dapsone, Clofazimine. PB gets R+D (6 months). MB gets all three (12 months).
- SJS < 10% BSA; TEN > 30% BSA. Most common drugs: sulfonamides, carbamazepine, allopurinol, phenytoin.
- Thalidomide is the drug of choice for ENL (Type 2 lepra reaction). Absolutely contraindicated in pregnancy.
- Wickham striae + violaceous papules + flexor surface = lichen planus. Always test HCV serology.
- Examiners commonly test the "row of tombstones" description - this is the histopathological hallmark of pemphigus vulgaris (basal cells attached to dermis after suprabasal split).
For topic-wise QBank practice, check the PrepLadder app.
Frequently Asked Questions
What is the difference between pemphigus and pemphigoid?
The key difference between pemphigus and pemphigoid lies in their distinct blistering mechanisms, which produce different types of blisters. The direct immunofluorescence test shows different results because pemphigus shows a fishnet pattern, while pemphigoid displays a linear pattern. Pemphigus represents a greater health risk, while pemphigoid occurs more frequently.
What is the first-line systemic drug for severe psoriasis?
In severe plaque psoriasis, the first-line treatment involves methotrexate, which doctors start at a weekly dosage of 7.5 to 15 milligrams. The drug works by blocking dihydrofolate reductase, which leads to T-cell activation suppression. The process requires doctors to track both liver function and complete blood count results. Acitretin acts as the primary treatment option for pustular psoriasis because it belongs to the retinoid drug family.
Which drug causes Stevens-Johnson Syndrome most commonly?
Among all medications, sulfonamides represent the drug class most likely to cause SJS, which occurs throughout the world. The other drugs that present a high risk for this condition include carbamazepine, allopurinol, phenytoin and nevirapine. The Southeast Asian population needs HLA-B*1502 testing before taking carbamazepine to assess their SJS susceptibility.
What is the Ridley-Jopling classification in leprosy?
In dermatology, the Ridley-Jopling classification divides leprosy into five types along an immunological spectrum: TT, BT, BB, BL, and LL. TT (tuberculoid) has strong cell-mediated immunity with few bacilli, while LL (lepromatous) shows immune anergy with high bacillary load. The borderline types remain unstable in their immune system function, which makes them vulnerable to immunological reactions.
Is vitiligo associated with other autoimmune diseases?
Indeed, vitiligo is most commonly associated with autoimmune thyroid disease, which develops in up to 20 per cent of patients, type 1 diabetes mellitus, pernicious anaemia, Addison's disease, and alopecia areata. NEET PG questions often present a vitiligo patient with fatigue and ask you to check thyroid function tests.
How is dermatology tested in NEET PG?
In NEET PG exams, dermatology questions typically present a clinical scenario with 2-3 key findings.
Pemphigus causes flaccid, intraepidermal blisters due to acantholysis (antibodies against desmogleins), while pemphigoid causes tense, subepidermal blisters (antibodies against basement membrane antigens BP180/BP230). DIF distinguishes them: fishnet pattern in pemphigus, linear pattern in pemphigoid. Pemphigus is more dangerous; pemphigoid is more common.
CLINICAL PEARL
In dermatology, the skin is where diagnosis begins, while histology and immunofluorescence results provide diagnostic answers. The clinical photo requires your visual training, while the microscope requires you to develop memory skills for its operation.
After 10 years of observing students tackle dermatology, I can tell you that the students who score highest on exams build comparison tables in their heads, while the students who memorise isolated facts score lower.

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
Why Dermatology Is a Scoring Gold Mine in NEET PG
Vesiculobullous Disorders - Pemphigus vs Pemphigoid
Pemphigus Vulgaris:
Bullous Pemphigoid
Psoriasis - Pathogenesis, Types & Treatment Ladder
Treatment Algorithm:
Ridley-Jopling Classification
WHO-MDT Regimen
Lepra Reactions (Exam Favourite)
Lichen Planus - The 6 Ps and Variants
Pigmentary Disorders - Vitiligo & Melasma
Master Comparison Table: Top Dermatology Conditions for NEET PG
High-Yield Points for NEET PG
Frequently Asked Questions
What is the difference between pemphigus and pemphigoid?
What is the first-line systemic drug for severe psoriasis?
Which drug causes Stevens-Johnson Syndrome most commonly?
What is the Ridley-Jopling classification in leprosy?
Is vitiligo associated with other autoimmune diseases?
How is dermatology tested in NEET PG?
CLINICAL PEARL
Top searching words
The most popular search terms used by aspirants
- Medical PG Dermatology
- NEET PG Dermatology