Abdominal Trauma in Pregnancy - Surgery
Apr 12, 2023

Abdominal trauma is a common and potentially life-threatening condition that requires urgent surgical intervention. Understanding the evaluation, management, and surgical techniques involved in treating abdominal trauma is essential for medical aspirants.
In the NEET PG exam, there are often questions related to abdominal trauma, including the mechanism of injury, diagnostic workup, surgical approach, and postoperative care. Therefore, having a good understanding of this important surgery topic and its management is crucial for success in the NEET PG exam, as well as for providing safe and effective surgical care in clinical practice.
Read this blog further for a quick overview of this important topic.
FAST, DPL (Diagnostic Peritoneal Lavage) ,
One liner on Abdominal trauma
- Most commonly injured organ in BTA - spleen > liver
- Most commonly injured organ in penetrating trauma - liver > stomach > SI
- Most commonly injured part of bowel in BTA – Jejunum
- Most commonly injured organ in Gunshot injury – Small intestine
- Most commonly site of injury in deceleration injury – Duodenojejunal junction
- Most commonly injured structure in seat belt injury - Mesentery
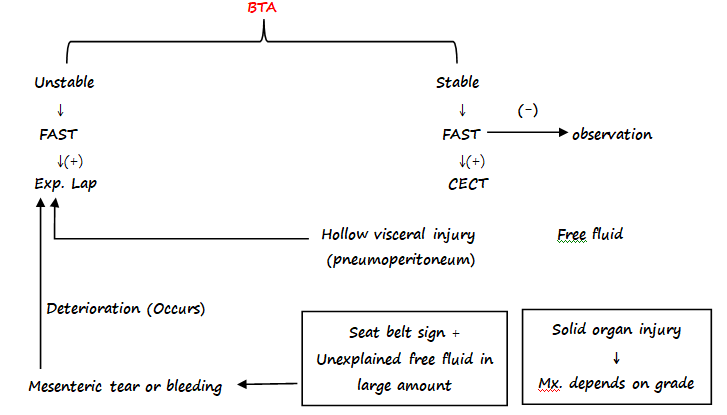
- 1st inv. Done in patient of BTA - FAST
- Gold standard investigation for stable patient of BTA - CECT
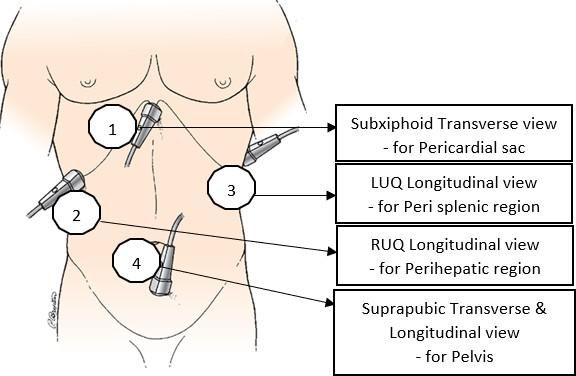
FAST (Focused Assessment with Sonography for Trauma)
- It is an Emergency ultrasound i.e. performed very fast [in 2 – 4 minutes]
- Assess Potential sites of thoracoabdominal injuries (4P’s) - Pericardial sac
- Perihepatic region
- Peri-splenic region
- Pelvis
- 4 traditional views in FAST
e - FAST (extended FAST)
- Has two additional views (so, has a total of 6 views)
- Right thoracic view
- Left thoracic view
- Pneumothorax on e-FAST shows barcode sign / stratosphere sign
Previous Year Question
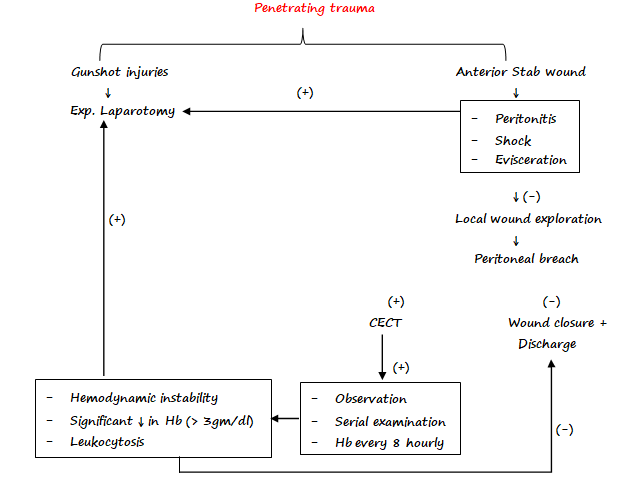
Q. A patient with stab injury to anterior abdomen presents with a tag of ometum protruding through the abdominal wall near the umbilicus. On evaluation he is haemodynamically stable and shows no signs of peritonitis. Initial management of patient involve:
- FAST
- Exploratory laparotomy
- Local wound exploration and suturing
- CECT abdomen.
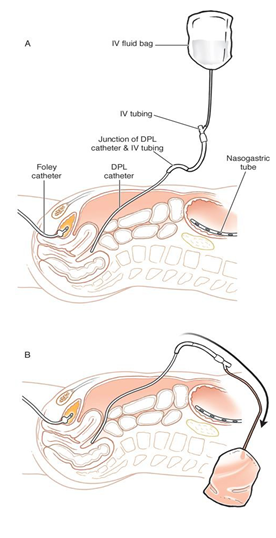
DPL (Diagnostic Peritoneal Lavage)
- Performed for BTA patients
- Catheter is inserted after infra umbilical incision & director towards pelvis
- Aspiration is done
- Instill IL of NS / RL →for lavage
- Re-aspiration of fluid is done
↓
This fluid is sent for examination
This fluid is sent for examination
- DPL is considered (+) ve
- 10 ml of frank blood is aspirated
- Returned effluent contain:
- RBCs →> 1 Lac/ mm3
- WBCs →> 500/ mm3
- Presence of bile, bacterial, fecal matter, vegetable matter
- Amylase > 175 IU / dl
Previous Year Question
All of the following are suggestive of positive DPL except:
- >10 ml of gross blood is aspirated directly from peritoneal cavity.
- Effluent contains RBCs> 1 lac/ cubic mm
- Effluent contains amylase>174IU/dl
- None of the above.
PENETRATING TRAUMA
- MC injured organ - liver > stomach > SI
- MC injured organ in GSW – SI
- Exp. Lap is mandatory - GSW (Gunshot wound)
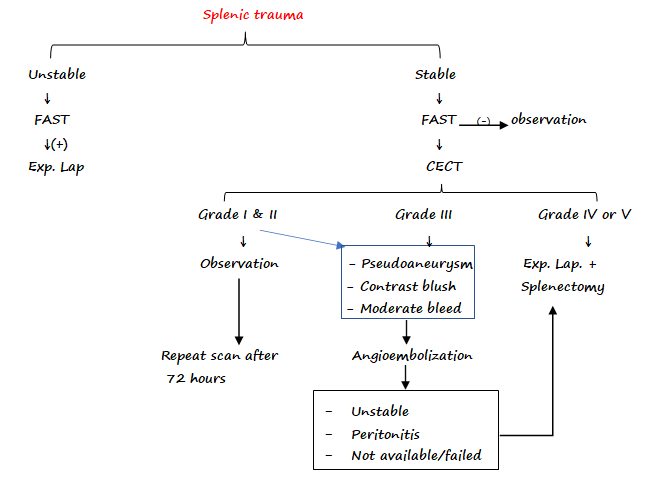
Splenic trauma
- MC injured organ in BTA
- Kehr’s sign
- Pain is referred to tip of Left shoulder in splenic rupture
- Due to irritation of undersurface of diagram with blood →pain is referred to shoulder via fibers of phrenic nerve (C4, C5)
- Ballance sign
- Fixed area of percussible dullness in LUQ due to coagulation of blood
AAST Grading for splenic trauma (American Association for Surgery of trauma)
Grade Hematoma Laceration I Subcapsular hematoma involving < 10% surface area Capsular tear < 1 cm in depth II S/C hematoma involving10 – 50 % Surface area 1 – 3 depth III S/C hematoma involving>50 % Surface area > 3 cm or involving Trabecular vessels IV > 25% devascularization Laceration involving Hilar vessels V Completely shattered spleen Complete devascularization
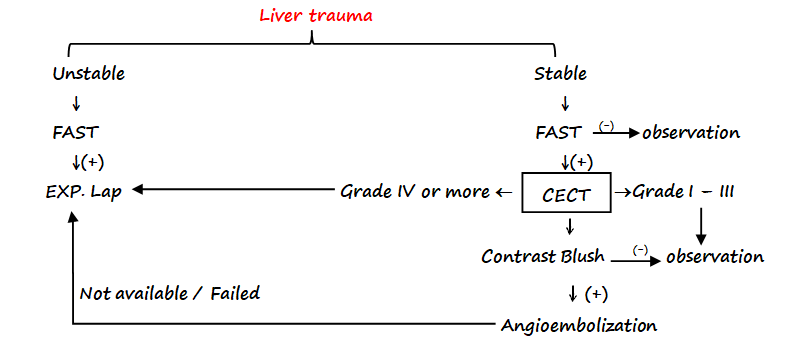
Liver Trauma
- MC injured organ in penetrating trauma
- 2nd MC injured organ in BTA
- Most liver injuries involve - segment 6, 7, 8
- Bleeding - mainly venous →low pressure tamponade is readily performed
- 4 ‘p’s in liver injury
- Push
- Plug
- Pringle
- Pack
Bear claw laceration - multiple linear lacerations of liver on CECT
PRINGLE’s Maneuver
- aka Total Inflow Occlusion
- Non-traumatic clamping in the foramen of Winslow and we occlude the Portal triad.
- It controls bleeding from Portal Vein and Hepatic Artery.
- Bleeding is effectively controlled from Portal Vein as compared to Hepatic Artery.
- It doesn’t control bleeding from IVC and Hepatic Vein
AAST →Grading of liver trauma
Grade Hematoma Laceration I Subcapsular hematoma involving < 10% surface area Capsular tear < 1 cm in depth II S/C hematoma involving 10 – 50 % Surface area 1 – 3 cm depth III S/C hematoma involving >50 % Surface area > 3cm depth IV - Parenchymal disruption involving 25-75% of hepatic lobe V - Parenchymal disruption involving >75% of hepatic lobe VI Hepatic avulsion
DUODENAL TRAUMA
- A/W pancreatic injuries
- IOC for Dx of Duodenal trauma – CECT
- On radiological Ix only sign is seen - gas or fluid in R/P & leakage of oral contrast
- Injury of 1st, 3rd or 4th part - repaired like small bowel with sutures
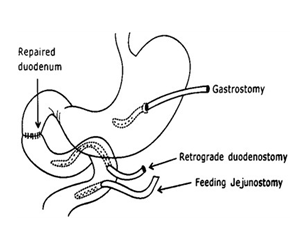
- Injury of 2nd part – Damage control surgery (Triple tube ostomy)
- Triple tube ostomy
- Decompressive Gastrostomy
- Decompressive Duodenostomy
- Feeding Jejunostomy
PANCREATIC TRAUMA
- In adult: MC cause – Penetrating
- In children: MC cause - Blunt trauma
- Handlebar → bicycle
- MC affected → body of pancreas
| Grade | Hematoma | Laceration |
| I | Minor contusion without duct injury | Superficial laceration without duct injury |
| II | Major contusion without duct injury | Major laceration without duct injury |
| III | - | Distal transection or parenchymal injury with duct injury |
| IV | - | Proximal transection or parenchymal injury involving Ampulla |
| V | - | Massive disruption of pancreatic head |
Diagnosis
- IOC for Dx – CECT
- ERCP - Most reliable test to demonstrate pancreatic duct integrity
Management
- I – Observation
- II – Debridement, drainage, possible repair
- III – Distal resection, Roux-en-Y drainage
- IV & V - Damage control surgery
- Résection + Roux-en-Y drainage
- Triple tube decompression
- Pyloric exclusion
- Duodenal diverticulization
- PancreaticoDuodenectomy
- MC complication seen after Pancreatic trauma - Pancreatic fistula / Persistent drain output
Also Read :
SEAT BELT INJURY
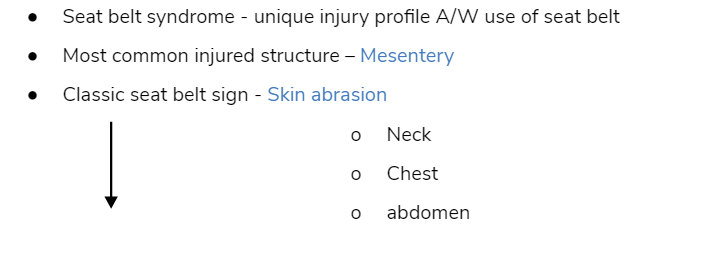
Associated with
- High chances of internal organ injury
- Also associated with pancreatico-Duodenal injuries
- Longitudinal mesentery tear – Repair
- Transverse mesentery tear – Resection & anastomosis
Trauma Triad of death
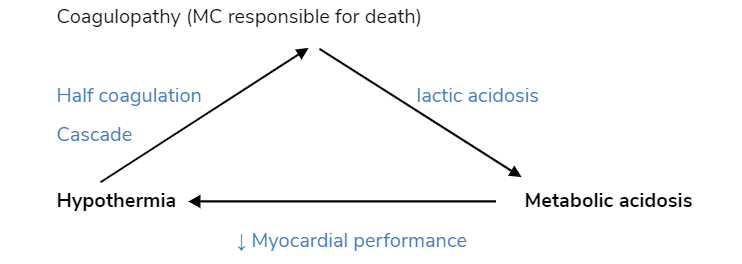
Hypothermia Metabolic acidosis
↓ Myocardial performance
Damage control surgery (DCS)
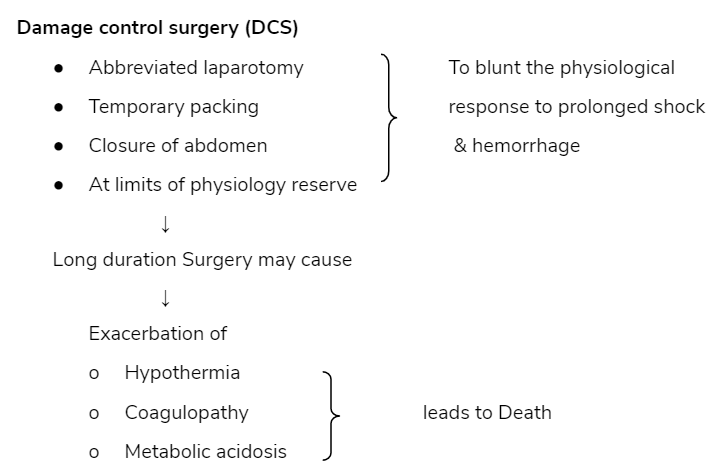
Phase of Damage control surgery
|
Phase I (initial exploration) |
Phase II (20 resuscitation) |
Phase III (Definitive operation) |
↓
↓ Segmental Stapled resection |
↓ For 2° resuscitation
|
|
Stage of DCS
- Stage I → Patient selection
- Stage II → Operative control of hemorrhage and contamination
- Stage III → ICU resuscitation
- Stage IV → Definitive surgery
- Stage V → Abdominal closure
Abdominal compartment syndrome (ACS)
- ACS – ↑sed IAP (>20 mmHg) – Results in compression of abdominal structures
- Causes fatal complications
- Pulmonary failure
- Mesenteric vascular compromise
- Normal IAP: 5-7 mmHg
- Intra-abdominal HTN ≥ 12 mm Hg
Predominantly occurs in
- Patients of profound shock
- Patients requiring large amount of fluid or blood for resuscitation
- Major visceral or vascular abdominal injuries
C/F
- Sudden increase in IAP
- ↑ peak inspiratory pressure
- Hypoxia, hypercapnia, hypotension
- ↓sed Venous return to heart
- ↓sed Urine output
Physiological consequence of ACS
|
Decreased |
Increased |
↓ ↓ VBF (Visceral blood flow)
|
Hypercapnia
|
Diagnosis
- Measure Bladder pressure -as it represents IAP
- Gold standard indirect method to measure IAP -Urinary bladder catheter
Management (depends on grade)
|
Grade |
Bladder pressure (mmHg) |
C/F |
Rx |
|
I |
12 – 15 |
None |
Normovolemic resuscitation |
|
II |
16-20 |
Oliguria, Splanchnic Hypoperfusion |
Hypovolemic resuscitation |
|
III |
21 – 25 |
Anuria, increased Ventilation pressure |
Decompression |
|
IV |
> 25 |
Anuria, increased ventilation pressure + ↓PO2 |
Emergency re exploration |
Pressure according to grade
- I →<10 – 15 cm H2O
- II →< 16 – 25 cm H2O
- III →< 26 – 35 cm H2O
- IV →> 36 cm H2O
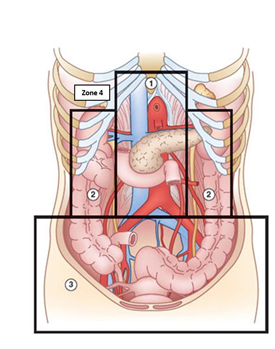
RETRO PERITONEAL INJURIES
Zone I – Central
- Extends from Esophageal hiatus to sacral promontory
- Hemorrhage or hematoma - usually located in midline
- A/W injuries of
- Aorta & its proximal branches
- IVC & its proximal tributaries
- It is divided into
|
Supra mesocolic Zone 1 |
Infra mesocolic Zone 1 |
|
|
|
their bifurcation |
Management
- Central hematoma – exploration with proximal & distal vascular control
Zone 2 – lateral
- Extends from lateral diaphragm to iliac crest
- Structures located - Distal renal vessels
- Management
- Lateral hematoma (renal in origin) - Managed non-operatively (angio- embolization)
Zone 3- Pelvic
- Confined to retroperitoneal Zone of pelvis
- Structures located - Iliac vessels
- Management
- Pelvic hematoma - Exceptional difficult to control
- Usually it should not be opened
- Packing / Angio-embolization
Zone 4 - Portal & retro hepatic areas
RENAL TRAUMA
- MC injured part of urinary tract – Kidney
- MC cause of renal trauma – RTA
- Best predictor of traumatic urinary system injury - Hematuria
Diagnosis
- IOC for Dx of renal injuries in stable patient – CECT
- IOC for Dx of renal injuries in unstable patient - single shot IVP (Assess function of C/L kidney)
Grading of Renal Trauma
|
Grade |
Description |
|
1 |
|
|
2 |
|
|
3 |
|
|
4 |
|
|
5 |
|

Management of Renal Trauma
- >95% of cases → Conservatively (low grade injury)
- < 5% of cases → Operative intervention
Indications of Renal exploration
Absolute Relative Persistent renal bleeding
Expanding or Pulsatile perirenal hematomaUrinary extravasation
Non-viable tissue
Segmental arterial injuries
Indications of Nephrectomy
- Unstable pt. → hypothermia / coagulopathy with normal contralateral kidney
- Extensive renal injury
- Poor functioning hydronephrotic kidney
Expand your understanding of this important Surgery topic with our engaging video lectures by Dr Pritesh Singh. Download the PrepLadder app and get access to high-quality preparation resources for NEET PG exam.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
FAST, DPL (Diagnostic Peritoneal Lavage) ,
One liner on Abdominal trauma
FAST (Focused Assessment with Sonography for Trauma)
DPL (Diagnostic Peritoneal Lavage)
This fluid is sent for examination
PENETRATING TRAUMA
Splenic trauma
AAST Grading for splenic trauma (American Association for Surgery of trauma)
Liver Trauma
PRINGLE’s Maneuver
AAST →Grading of liver trauma
DUODENAL TRAUMA
PANCREATIC TRAUMA
Diagnosis
Management
SEAT BELT INJURY
Associated with
Trauma Triad of death
Hypothermia Metabolic acidosis
Damage control surgery (DCS)
Phase of Damage control surgery
Abdominal compartment syndrome (ACS)
Predominantly occurs in
C/F
Physiological consequence of ACS
Pressure according to grade
RETRO PERITONEAL INJURIES
Zone I – Central
Management
Zone 2 – lateral
Zone 3- Pelvic
Zone 4 - Portal & retro hepatic areas
RENAL TRAUMA
Diagnosis
Grading of Renal Trauma
Management of Renal Trauma
Indications of Renal exploration
Indications of Nephrectomy
Top searching words
The most popular search terms used by aspirants
- Medical PG Surgery
- NEET PG Surgery
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial