Alcoholic Liver Disease: Symptoms, Diagnosis, Treatment & Risks
Nov 13, 2024

Overview of alcohol-associated liver disease
Alcoholic-associated Liver Disease
- Alcohol and its impact on the liver—the whole manifestations are labeled as alcoholic liver disease.
- This broad term has been replaced in most of the guidelines, like European and American, as alcoholic-associated liver diseases.
- Spectrum of the alcohol-induced liver disease:
- Acute liver injury
- Chronic liver injury
Chronic Liver Injury
- Steatosis - fat degeneration
- Steatohepatitis - steatosis + inflammation
- Cirrhosis - steatosis, and steatohepatitis both can cause fibrosis leading to cirrhosis.
- Complications: Decompensated liver disease, Hepatocellular carcinoma
Acute Liver Injury
- It is also known as alcoholic hepatitis.
- According to European guidelines, it is known as alcohol-associated hepatitis.
Clinical Features
- Increased alcohol consumption-Binge
- Chronic alcohol consumption (> 100 gms/day, 10-20 yrs)
- Jaundice
- Abdominal pain in the right upper quadrant
- Fever
- Differential diagnosis: acute viral hepatitis
Also read: Periarticular Disorders: Soft Tissue Rheumatism & Treatments
Diagnosis: 2018 American College of Gastroenterology Guidelines
- Rapid development of worsening of jaundice
- Total serum bilirubin > 3 mg / dL
- AST, ALT > 1.5 × ULN & <400 U/L
- AST/ALT ratio > 1.5. Also known as the Deritis ratio
- Documentation of heavy alcohol use until 8 weeks prior to symptom onset
- Exclude other causes
MCQ
Q1. AST/ALT ratio is high in
Ans. Alcoholic hepatitis
Reasons
- AST is a mitochondrial enzyme, and ALT is a cytosolic enzyme.
- Alcohol is a predominant mitochondrial toxin; thus, the AST level will be increased.
- Secondly, AST is not liver-specific. It will be present in other tissues like muscles, etc.
- Thus, there is a chance of increased AST levels due to leaking, resulting in more elevated levels of AST
- ALT is not profoundly elevated because it is dependent on an enzyme called pyridoxal phosphate.
- That supply is reduced in patients with chronic alcoholism due to malnutrition.
- That lack of pyridoxal phosphate results in decreased levels of ALT, ultimately leading to an elevated AST/ALT ratio.
- >3 is Alcohol-induced liver injury
- Documentation of heavy Alcohol consumption until 8 weeks before symptom onset
- Exclude other causes like
- Acute Viral Hepatitis
- Proper history causing Drug-induced liver disease at least 30 days from onset of symptoms
- In 2019, the American Association for Liver Disease Guidelines mentioned following the 2016 consensus guidelines for diagnosis. According to this, there are three types of confidence.
Also read: Recurrent and Autoimmune Pancreatitis
Clinical Diagnosis of AH
- Onset of jaundice within the prior 8 weeks
- Ongoing consumption of >40 (female) or 60 (male) g alcohol/day for >6 months, with <60 days of abstinence before onset of jaundice
- AST>50, AST/ALT> 1.5, and both values <400 IU/L
- Serum total bilirubin >3.0 mg/dL
Potential Confounding Factors:
- Possible ischemic hepatitis (e.g., severe upper gastrointestinal bleed, hypotension, or cocaine use within 7 days or metabolic liver diseases like Wilson disease and alpha 1 antitrypsin deficiency)
- Possible drug-induced liver disease (suspect drug within 30 days of onset of jaundice)
- Uncertain alcohol use assessment (e.g., patient denies excessive alcohol use)
- Presence of atypical laboratory tests (e.g., AST <50 or >400 IU/L, AST/ALT <1.5), ANA >1:160, or SMA >1:80.
Prognostic Scoring:
- Modified Maddrey Discriminant Function Score (MMDF)
- Assessing the prognosis of Alcoholic hepatitis
- Predictor of mortality
- >32, steroids are given
- Components
- PT
- Serum bilirubin levels
Modified Maddrey Discriminant Function Score (MMDF)
Correlation on the Maddrey Discriminant function (DF)* with Prognosis in Alcohol-Associated
Hepatitis
| Disease Severity | Non-Severe Disease | Severe Disease |
| Score | <32 | ≥32 |
| Short-term Mortality Rate (%) | 10% | 30-60% |
| Glucocorticoid Therapy Indicated | No | Yes |
*DF= {4.6 ×[prothrombin time (sec)- control prothrombin time (sec)]}+ (serum bilirubin [mg/dL])
Also read: Menetrier's Disease: Epidemiology, Etiopathogenesis
MELD score
- Components
- Creatinine
- Bilirubin
- INR
- Steroid therapy >21
Correlation of the MELD score* with 3-month Mortality Rate in alcohol-associated hepatitis
| Score | 3-Month Mortality Rate (%) |
| 22 | 10% |
| 29 | 30% |
| 33 | 50% |
| 38 | 80% |
*MELD = (0.957 × log [creatinine]+0.378 × log [bilirubin]+1.12 × log [INR]+0.643)×10.
ABIC
- Components
- Age
- Bilirubin
- INR
- Creatinine
- Steroid therapy >9
ABIC score
Correlation of the ABIC Score and the 90-day Mortality Rate in Alcohol-Associated Hepatitis
| Severity | 90-Day Mortality Rate (%) |
| Low (<6.71) | 0% |
| Intermediate (6.71 - 8.999) | 30% |
| High (≥9.0) | 75% |
*ABIC score = (age × 0.1) + (serum bilirubin × 0.08) + (serum creatinine × 0.3) + (INR × 0.8)
Glasgow Alcohol-Associated Hepatitis score
- Components
- Age
- WBC
- BUN
- INR
- Steroid therapy >9
PYQ
Q2. Which scoring has WBC?
Ans. Glasgow Alcohol-Associated Hepatitis score
Also read: Mesenteric Ischemia: Causes, Symptoms, and Treatments
Management of Alcoholic Liver Disease
- Steroids - Improved short-term mortality
- Pentoxyphylline reduces the risk of Hepatorenal syndrome
- Steroids + N-Acetyl cysteine improve mortality
- Last half a decade, trials are done using
- Anabolic steroids
- Antioxidants
- Colchicine, lecithin
- Propyl thio uracil
- S-Adenosine methionine.
- All these drugs are not beneficial.
Management Algorithm
- History of alcohol consumption
- Lab profile
- Rule out Viral hepatitis markers
- Drug history
- Medical history
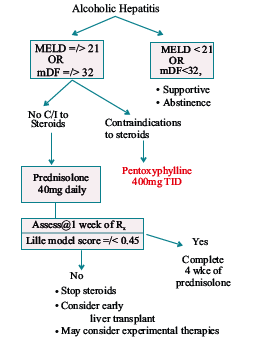
- Mild—not necessary to use steroids.
- Severe - necessary to use steroids with or without N-Acetyl cysteine.
- Contraindications to steroids:
- Active infections
- Decompensated liver disease
- Hepatorenal syndrome
- Active GI bleed
- Patients with no contraindications can be started with steroid therapy
.jpg)
Lille model score
The Lille Model Score Parameters
- Age
- Albumin
- Bilirubin (initial)
- Bilirubin level (day 7)
- Creatinine
- Prothrombin time
*The Lille score 3.19-0.101 (age [yrs])+0.147 (serum albumin [g/L])+ 0.0165 (change in serum bilirubin at day 7)- 0.206 (serum creatinine [mg/dL])-0.0065 (baseline serum
bilirubin [mg/dL])-0.0096 (prothrombin time [sec]) The score at 7 days determines response to treatment. A score of <0.45 is associated with a 15% mortality rate at 6 months.
PYQ
Q3. Albumin is a parameter in
Ans. Lille model score
- <0.45 score indicates steroid responsive
- Complete steroid course for 4 weeks
- Then taper dose for 2 weeks
Also read: Drug-Induced Liver Injury
2019 Alcohol-associated liver disease guidance statements
- Prednisolone (40 mg/day) given orally should be considered to improve 28-day mortality in patients with severe AH (MDF ≥32) without contraindications to the use of corticosteroids.
- The addition of intravenous N-acetyl cysteine to prednisolone (40 mg/day) may improve the 30-day survival of patients with severe alcoholic hepatitis.
- The Lille score should be used to reassess prognosis, identify non-responders, and guide treatment courses after 7 days of corticosteroids.
- Patients with alcoholic hepatitis should have malnutrition addressed and treated, preferably with enteral nutrition.
- Abstinence is key to long-term survival; methods discussed previously for the treatment of alcohol use disorders (AUD) should be used to increase abstinence.
- Pentoxiphilline is no longer recommended in the treatment of alcoholic hepatitis.
Hope you found this blog helpful for your NEET SS Gastroenterology and Hepatobiliary preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Alcoholic-associated Liver Disease
Chronic Liver Injury
Acute Liver Injury
Clinical Features
Diagnosis: 2018 American College of Gastroenterology Guidelines
MCQ
Clinical Diagnosis of AH
Potential Confounding Factors:
Prognostic Scoring:
Modified Maddrey Discriminant Function Score (MMDF)
MELD score
ABIC
Glasgow Alcohol-Associated Hepatitis score
PYQ
Management of Alcoholic Liver Disease
Management Algorithm
Lille model score
The Lille Model Score Parameters
PYQ
2019 Alcohol-associated liver disease guidance statements
Top searching words
The most popular search terms used by aspirants
- NEET SS Medicine Gastroenterology and Hepatobiliary Preparation
PrepLadder 4.0 for NEET SS
Avail 24-Hr Free Trial