Neonatal Jaundice - NEET PG Pediatrics
May 5, 2023

The most typical condition in neonates that needs medical treatment and hospital readmission is jaundice. Unconjugated bilirubin accumulates in jaundiced newborns, turning their skin and sclera yellow. Unconjugated hyperbilirubinemia in most babies indicates a typical developmental condition. Unconjugated bilirubin is neurotoxic and can result in both newborn death and permanent neurologic aftereffects (kernicterus) in children who survive. As a result, certain infants may experience significant increases in serum bilirubin levels. [89] These factors make diagnostic testing common when neonatal jaundice is present. In 60 % of term neonates & 80% of preterm neonates have clinical jaundice in 1st week of life. Clinical jaundice in neonates is seen at bilirubin level > 4- 6 mg/dlM/c/c of readmission of a neonate discharged from a hospital: Neonatal jaundice M/c/c of neonatal morbidity in 1st week is Neonatal Jaundice.
Read this blog further to get a quick overview of this important topic for pediatric preparation and ace your NEET PG exam preparation

Types of Jaundice
Physiological Jaundice
In this the Icterus/clinical jaundice never appear in 1st 24hrs of life. It is Always unconjugated i.e urine does not stain diapers and no pale stools will be seen Palms and soles never stained yellow. Clinical jaundice doesn’t persist beyond 2 weeks in term neonates and 3 weeks in preterm neonates
Pathological jaundice
Clinical jaundice may appear in the 1st 24 hrs of life. It May be conjugated/unconjugated. High coloured urine; pale stools may or may not be seen.Palms and soles may be stained yellow. May persist beyond 3 weeks.
Breastfeeding jaundice
It occurs due to inadequate Breastfeeding which leads to Dehydration and also Relative polycythemia. Higher bilirubin level as due to increased polycythemia there will be excessive breakdown of hemoglobin into bilirubin. Treatment of breastfeeding jaundice is Frequent breastfeeding.

Breast Milk Jaundice
It occurs due to substances present in breast milk like pregnanediol & free fatty acids, that interfere with the conjugation of bilirubin treatment of breast milk jaundice is Continued breastfeeding. Breastfeeding may be temporarily withheld if bilirubin >20 mg/dl.
Causes of physiological jaundice :
Due to Higher production of bilirubin which is because of:
- Higher Hb level in neonates
- Shorter life span of RBCs (90 days vs 120 days).
- More ineffective erythropoiesis
- Ineffective carrier mediated uptake of bilirubin by liver
- Immature UDP Glucoronyl transferase enzyme activity
- Increased enterohepatic circulation in neonates
Causes of pathological jaundice
A. Unconjugated Hyperbilirubinemia
- Increased Production of Bilirubin
- Hemolytic disorders like :
- a) Erythroblastosis fetalis [Hemolytic disease of newborn]: Hemolytic anemia in the fetus known as erythroblastosis fetalis is brought on by the transplacental transfer of maternal antibodies to fetal red blood cells. This condition is typically brought on by incompatibility between the maternal and fetal blood groups, frequently Rho(D) antigens. It is the cause of neonatal jaundice which occurs during first 24 hrs of life
- b) Hereditary spherocytosis: Blood condition known as hereditary spherocytosis is inherited. The red blood cells (RBCs) are the cause of this issue. The cells have a sphere-like form rather than a disk-like shape.
- c) G6PD deficiency: A hereditary condition called glucose-6-phosphate dehydrogenase deficiency affects red blood cells, which are responsible for transporting oxygen from the lungs to all of the body's organs. Red blood cells in those who are affected prematurely degrade due to a glucose-6-phosphate dehydrogenase enzyme deficiency.
- d) Polycythemia: A primary or secondary condition characterized by an unusually high concentration of red blood cells in the blood, typically linked to heart or lung disease or high altitude residence.
- e) Cephalhematoma: An accumulation of blood under the scalp, more precisely in the sub-periosteal region, is known as a cephalohematoma. Blood vessels rupture as a result of the periosteum being torn away from the underlying calvarium during the birthing process, which involves shearing forces on the skull and scalp.
- f) Infant of diabetic mother
- g) Delayed cord clamping
- Decreased Conjugation of Bilirubin
- a)Crigler Najjar syndrome -UDP- glucuronosyltransferase, an enzyme necessary for the glucuronidation of unconjugated bilirubin in the liver, is absent or has diminished activity in Crigler-Najjar syndrome, a rare autosomal recessive hereditary illness. Congenital non-hemolytic jaundice has this as one of its main causes.
- Type I: Complete deficiency of UDP-glucuronosyltransferase
- Type II: Partial deficiency of UDP-glucuronosyltransferase
- Treatment: phenobarbitone as it an enzyme inducer it increases the production of UDP-glucuronosyltransferase
- b)Gilbert syndrome- Gilbert syndrome is an autosomal recessive condition that affects the liver's ability to process bilirubin. Unconjugated hyperbilirubinemia and recurrent jaundice are caused by reduced glucuronidation of bilirubin.[1] In typical conditions, roughly 95% of bilirubin is unconjugated.
- c)Down syndrome
- d)congenital hypothyroidism
B. Conjugated Hyperbilirubinemia -
We considered it when the Conjugated Bilirubin Is more than 2 mg/dl or it is more than 20% of total bilirubin
Non-Obstructive Causes
- Infections such asViral: EBV, CMV, hepatitis ,Bacterial: Congenital TB in this the Ghon focus seen in liver and Parasitic such as Toxoplasmosis
- Toxins -Sepsis, UTI, TPN
- Metabolic
- Tyrosinemia
- Galactosemia
- Hereditary fructose intolerance
- Alpha 1 antitrypsin deficiency
- Cystic fibrosis
- Idiopathic neonatal hepatitis
- MC cause of conjugated hyperbilirubinemia in neonates
Obstructive Causes
Intra Hepatic Causes
- Congenital hepatic fibrosis
- Caroli’s disease
- Progressive familial intra hepatic cholestasis
- Alagile syndrome(bile duct paucity syndrome)- In this we find Triangular facies and Butterfly shaped vertebrae
- Pulmonary stenosis
- Dubin Johnson syndrome
- Pigmented liver(Dark liver)
- Rotor syndrome
Extra Hepatic Causes
- Extra hepatic biliary atresia (EHBA)-Screening test for EHBA: HIDA Scan (or) hepatic scintigraphy
- Surgery for EHBA is known as KASAI Procedure [portoenterostomy]. favorable results if done < 8 weeks of life
- EHBA is the MC indication for liver transplantation in children
- Choledochal cyst
- Stones
- Stricture
- Mass
Clinical Features of Neonatal Jaundice
Ways to detect neonatal jaundice is by Clinical examination that can be done by Modified Krammer's rule or with the help of Transcutaneous bilirubinometer this method Avoids blood sampling but it is : Not very reliable in
a. During first 24 hours of life
b. Gestational age <35 weeks
c. Baby on phototherapy
d. Bilirubin >12-14 mg/dl
- Serum bilirubin level
Pediatrics Related Articles:
Modified Krammer’s Rule
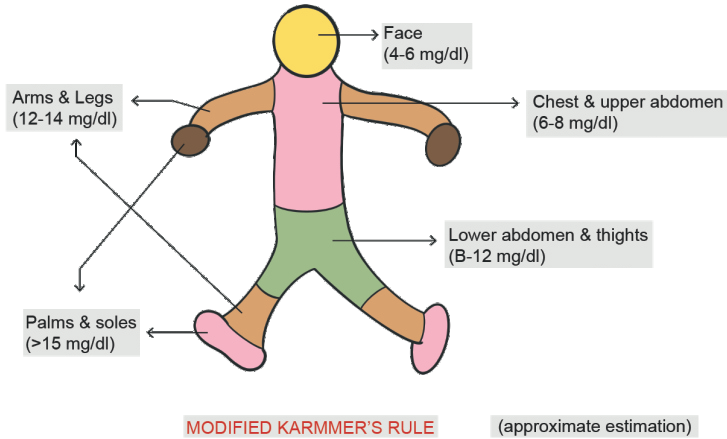
Lemon Yellow(mg/dl) Orange Yellow(mg/dl) Face 5-7 7-9 Chest and upper abdomen 7-9 9-11 Lower abdomen and thighs 9-11 11-14 Arm and legs 11-13 14-16 Palms and soles 13-15 >/=17
Neurological Manifestations
Most Commonly involved part of brain in neonatal jaundice: Basal ganglia Type of cerebral palsy seen: Extra pyramidal type Kernicterus is Yellow staining of basal ganglia.
Acute Bilirubin Encephalopathy
- Early features [mild]: Hypotonia, poor feeding, loss of moro's reflex which leads to Fever, irritability, seizures.
- Features of Advanced disease (severe): Hypertonia, Opisthotonic posturing, coma, death.
Chronic Bilirubin Encephalopathy
- Mnemonic: SADMUM
- S - Sensorineural hearing loss
- A - Athetosis
- D - Dental dysplasia dental enamel changes)
- M - Mental retardation
- U - Upward gaze limitation
Treatment of Neonatal Jaundice
- I. Phototherapy
- II. Exchange transfusion
- III. Drugs
Exchange Transfusion
- It is Used in very severe cases, especially Erythroblastosis Fetalis . Double volume exchange transfusion is done i.e the transfusion is done with the double amount of blood that is present in the body.
Drugs
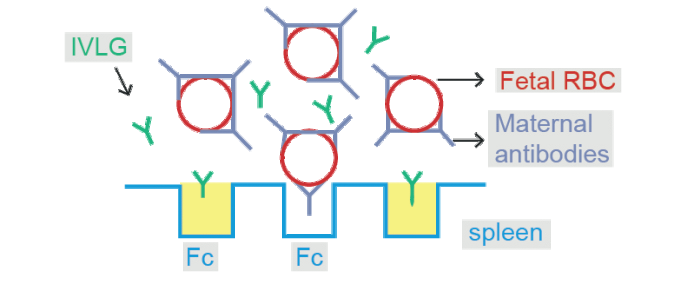
- IV Ig (Intravenous immunoglobulin) - Used in Erythroblastosis fetalis . It Occupies the receptors for FC segment of Ig in reticuloendothelial system & prevents further production of Ig
- Phenobarbitone
Severe Neonatal Jaundice Due to Erythroblastosis Fetalis the Treatment Order should be as
Start Phototherapy
↓
Do exchange transfusion
↓
IVIg
Phototherapy
Most effective wavelength of light used 460-490 nm.
Mechanisms by Which Phototherapy Acts
- 1. Photo Isomerisation ; In this the Bilirubin is converted into Polar compounds which are excreted through the kidney without conjugation. It is Slow & reversible process
- 2. Structural Isomerisation : In this the Bilirubin is converted into Lumirubin which is excreted through the kidney without conjugation. It is a Faster & irreversible so it is considered as Most important mechanism by which phototherapy acts .
- 3. Photo Oxidation [least important] ;Irradiance should be at least 30 micro W/cm 2/nm it is Measured using flux meter
Effectiveness of Phototherapy Depends Upon:
- Exposed surface area of baby
- Distance b/w baby & phototherapy unit [30-45 cm]
- Type of lamp used: LED lamps > CFL Lamps
Effectiveness does not depend on skin pigmentation of baby
Adverse Effects of Phototherapy
- Bronze baby syndrome
- Dehydration
- Watery diarrhea
- Hypocalcemia
- Retinal toxicity
- Gonadal toxicity or mutations
- Impaired maternal child bonding
In Healthy Term Neonates
| Age | Phototherapy Cut off | Exchange Transfusion Cut off |
| 24-48 hrs | >15 mg/dl | >20 mg/dl |
| 48-72 hrs | >18 mg/dl | >25 mg/dl |
| >72 hrs | >20 mg/dl | >25 mg/dl |
In Preterm Neonate
- Phototherapy cut off is 1% of birth weight in grams
- Exchange transfusion cut off is Phototherapy cutoff +5 [mg/dl]
- Indications of exchange transfusion in a baby with RH incompatibility is if the Cord blood Bilirubin: > 5 mg/dl or the Cord blood Hb is < 10 mg
This is everything that you need to know about hyperthyroidism for your pediatric preparation. For more interesting and informative blog posts like this download the PrepLadder App and keep reading our blog!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Types of Jaundice
Physiological Jaundice
Pathological jaundice
Breastfeeding jaundice
Breast Milk Jaundice
Causes of physiological jaundice :
Causes of pathological jaundice
A. Unconjugated Hyperbilirubinemia
B. Conjugated Hyperbilirubinemia -
Non-Obstructive Causes
Obstructive Causes
Intra Hepatic Causes
Extra Hepatic Causes
Clinical Features of Neonatal Jaundice
Modified Krammer’s Rule
Neurological Manifestations
Acute Bilirubin Encephalopathy
Chronic Bilirubin Encephalopathy
Treatment of Neonatal Jaundice
Exchange Transfusion
Drugs
Phototherapy
Effectiveness of Phototherapy Depends Upon:
Adverse Effects of Phototherapy