Oncologic Emergencies : Catheter Infection
Aug 14, 2024

Febrile Neutropenia(FN)
In layman's terms, it means Fever Neutropenia. Fever is when there is a single oral temperature ≥ 38.30 C (1010 F) C or ≥380 C (100.40 F) for ≥ 1 hour, and Neutropenia is when ANC < 500 or < 1000 with predicted nadir < 500
- Pathophysiology and microbiology of febrile Neutropenia
- Gram Positive Cocci (Most Common-70%). Fungal superinfection if prolonged neutropenia and antibiotic use.
- Gram-negative rods usually seed from GIT
- Predisposing factor of febrile Neutropenia
- Catheters, skin breakdown, GI mucositis, obstruction (lymphatics, biliary tract, GI/GU tract), immune defect in cancers.
- Clinical features of febrile Neutropenia
- If RLQ pain, watery/ bloody diarrhea+cecal wall thickening, consider neutropenic enterocolitis (typhlitis)
- Risk stratification of Febrile Neutropenia
- Risk can be assessed by the MASSC risk index. MASSC risk index ≥21 = low risk, < 21 = high risk
| Characteristics | Score |
| No or mild symptoms | 5 |
| No hypotension (SBP>90 mm HG) | 5 |
| No COPD | 4 |
| No H/o fungal infections | 4 |
| No dehydration requiring parenteral fluids | 3 |
| Outpatient status | 3 |
| Age<60 years | 2 |
Treatment of Febrile Neutropenia
- Antibiotics until FN resolves (Afebrile + ANC > 500)
- Cover GNR (including pseudomonas) + sensitive GPCs 1st
- Piperacillin-tazobactam: A broad-spectrum penicillin and beta-lactamase inhibitor combination that covers many Gram-negative and Gram-positive bacteria, including Pseudomonas.
- Carbapenems (e.g., Meropenem, Imipenem)
- Cefepime is a fourth-generation cephalosporin effective against many Gram-negative bacteria, including Pseudomonas, as well as susceptible Gram-positive cocci.
- Cover resistant GPCs if decreasing BP(Hypotension), PNA, mucositis, catheter/soft tissue infection
- Vancomycin: S/E-nephrotoxicity
- Linezolid: It belongs to a class of antibiotics known as oxazolidinones & is used to treat infections caused by Gram-positive bacteria, including those that are resistant to other antibiotics. S/E-Bone marrow suppression, thrombocytopenia, agranulocytosis & anemia
- Daptomycin - Ineffective in pneumonia. This is because daptomycin's mechanism of action makes it ineffective against bacteria in the presence of lung surfactants, which can be found in the lungs and respiratory system.
- Tigecycline - Cannot maintain blood levels. On the other hand, tigecycline is often considered a good option for treating gastrointestinal (GI) infections.
- Teicoplanin is often used as an alternative to vancomycin.It is used to treat infections caused by Gram-positive bacteria, including infections caused by methicillin-resistant Staphylococcus aureus (MRSA) and other resistant strains of bacteria.
- If no obvious infection site + continuing fever -> empirical antifungals
- Broad spectrum anti-fungal
- Voriconazole Voriconazole causes liver damage, monitor liver functions
- Liposomal Amphotericin B (LAMB)
- Echinocandins: The three main echinocandin drugs are Caspofungin, Micafungin, and Anidulafungin. Echinocandins are effective against certain types of Candida species, particularly those that cause invasive candidiasis and candidemia. However, they are generally not the first-line treatment for infections caused by Aspergillus species. LAMB: Nephrotoxic, so monitor renal functions
Also Read: Etiology Screening of Cancer
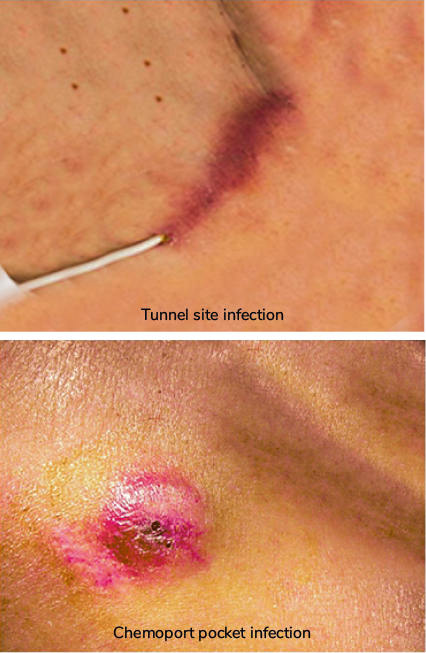
Catheter infection
GPCs most common: Staphylococcus aureus (MRSA/MSSA), CONS(Staphylococcus epidermidis)
| Situation | Catheter Removal | Comments |
| Negative culture | ||
| Exit site erythema | Not required | CONS are the MC organisms |
| Tunnel site erythema | Required | Can result in necrosis of the tunnel site |
| Positive cultures | ||
| CONS | Decide on case to case basis | Rx Vancomycin or Daptomycin |
| Other GPCs | Required | Treatment depends on culture reports |
| GNRs | Required | |
| Fungal | Required | Difficult to Treat |
 |  |
Metastatic Spinal Cord Compression
- Clinical manifestations of Metastatic Spinal Cord compression
- Metastases in the vertebral body extend and cause ESCC(Epidural spinal cord compression)

- MC cancers that metastasize
- Prostate, breast, and lung
- Site of involvement of Metastatic Spinal Cord compression
- Thoracic (60%) > lumbar (25%) > cervical (15%)
- Signs and symptoms of Metastatic Spinal Cord compression
- Pain (>95% MC) precedes neurologic symptoms (weakness, autonomic dysfunction, sensory loss)
Tumor Lysis Syndrome
- Types Of Tumor Lysis Syndrome
- Can be spontaneous or chemotherapy-related
- LTLS (≥2): increased K (≥6), increased UA (≥8), Increased PO4 (≥4.5): decrease in Ca (<=7) or 25% change
- CTLS (≥1): AKI, arrhythmias, Seizures, symptomatic hypocalcemia.
- Can be spontaneous or chemotherapy-related
- Treatment of Tumor Lysis Syndrome
- IVF, Rasburicase, correct electrolytes +/- RRT
- Prophylaxis of Tumor Lysis Syndrome
- IVF (0.9% or 0.45% NS 3L/m2/day) + Allopurinol 300 mg/m2 P/O (or) Rasburicase 0.2 mg/kg IV (C/I in G6PD deficiency) +/- RRT (if persistent TLS)
- Start chemo if S.UA > 8 and Serum creatinine < 1.6
- Consider early RRT for post-chemo TLS
- Risk Factors of Tumor Lysis Syndrome
| High Risk | Intermediate Risk | Low Risk |
| Burkitt lymphoma + LDH ≥2x | Burkitt lymphoma + LDH < 2x ULN | Indolent NHLs |
| DLBCL (Stage III/IV) + LDH ≥2x | DLBCL + LDH 1-2x ULN | HL |
| ALL + WBC ≥100K/LDH >= 2x | ALL + WBC < 100K + LDH < 2x ULN | MM and CML |
| AML + WBC >= 100K | AML + WBC < 100K + LDH < 2x ULN | AML + WBC < 25K + LD |
| CLL + LN >= 10 cm + High UA (or) ALC ≥25K + LN ≥5 cm | CLL + LN ≥ 5cm (or) ALC ≥25K | Most solid tumors |
| Solid tumors - SCLC, NB, GCT |
SVC Syndrome
Does not affect the cancer cure rates
- Etiology Of SVC Syndrome
- NSCLC > SCLC > Lymphomas > Mets > Others
- Clinical features Of SVC Syndrome
- Neck/face/arm edema, facial plethora, dilated neck/chest veins, laryngeal or cerebral edema, decreased BP
- Clinical diagnosis + confirmation with imaging
- Workup SVC Syndrome
- Venography (if severe) vs. CECT/MRI chest
- Treatment SVC Syndrome
- Supportive (HOB elevation +/- loop diuretic +/- Dexa)
- Endovascular Therapy (BA+stent) if severe (+/- lysis/AC if thrombus)
- Chemo/Radio-Therapy - definitive (depends on Biopsy and tumor type)
.jpg)
Frequently Asked Questions
Q: What does the NGS be considered to identify?
Answer: Actionable genomic aberrations
Q: Which drug cannot maintain blood levels but is good for GI infections?
Answer: Tigecycline
Q: Which antibiotic is completely ineffective in Pneumonia?
Answer: Daptomycin
Hope you found this blog helpful for your NEET SS Medicine Oncology preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.

Dr. Jaschandrika Rana
Dr. Jaschandrika Rana is a dedicated Medical Academic Content Writer with over 5 years of experience. She creates insightful and motivating content for medical aspirants preparing for the FMG Exam, Medical PG Exam, Residency courses, and the NEET SS Exam. Dr. Rana’s work inspires future medical professionals to achieve top ranks and excel in their careers.
Navigate Quickly
Febrile Neutropenia(FN)
Treatment of Febrile Neutropenia
Catheter infection
Metastatic Spinal Cord Compression
Tumor Lysis Syndrome
SVC Syndrome
Frequently Asked Questions
Top searching words
The most popular search terms used by aspirants
- NEET SS Medicine Oncology
PrepLadder 4.0 for NEET SS
Avail 24-Hr Free Trial