Complications of Renal Transplant
Nov 6, 2023

Early Graft Dysfunction
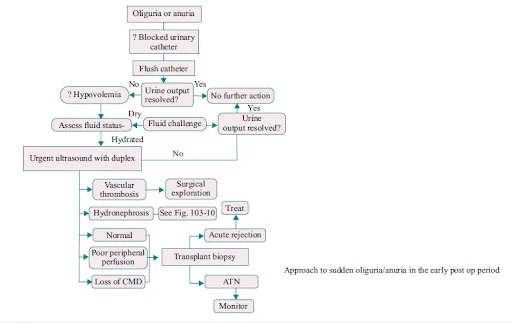
- Anuria/ oliguria (<50 ml/hr) in the postoperative period. Living donor transplants are always anticipated to have brisk urine output. Manage anuria aggressively. Clinical assessment (volume status and patency of catheter). USG Doppler to assess vascularity of graft. If Doppler is inconclusive - can go ahead with DTPA/ MAG3 scan.
Urologic Complications
Urine Leaks And Urinomas
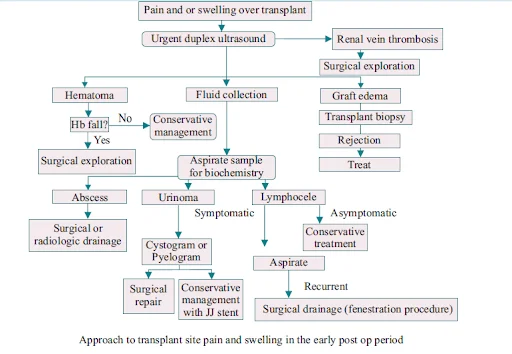
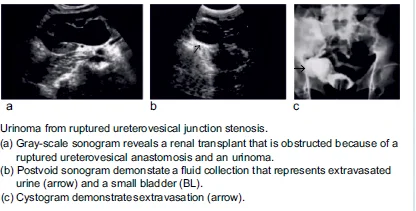
- Most common etiologies: Failure of ureterovesical anastomosis. Necrosis of the distal ureteric stump. Clinical signs: Decrease in urine output, fullness and tenderness around the graft, ipsilateral leg scrotal or labial swelling. USG features: Well-defined, anechoic, no septations, increase in size rapidly. USG guided drainage: Fluid creatinine high (Drain Fluid Creatinine/ DFC comes out to be around 10 times as compared to serum creatinine. This confirms that the extravasated fluid is urine and not some serous collection produced by the body.) Small urine leaks: PCN and stent placement, drain placement – evacuate urinoma, In these cases, the patient is put on antibiotic prophylaxis to prevent occurrence of infection. DJ Stent kept for 6-8 weeks (To allow the healing process to occur.) Large/ persistent leak: Reimplantation of the ureter, Pyelocystostomy or pyeloureterostomy with the native ureter.
Ureteral Obstruction
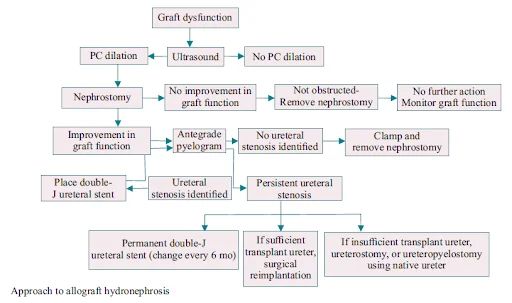
- Early obstruction: Edema, blood clots, hematoma, and kinking. Late obstruction: Fibrosis from chronic ischemia. Extraluminal (compression from lymphocele or spermatic cord). Ureteral (ischemia). Intraluminal (stone, fungal ball, sloughed renal papilla, foreign body). Presentation – elevated serum creatinine level. Allograft denervated – no renal colic. Diagnosis: USG graft: Hydronephrosis (HDN), Furosemide renogram: delayed images (2-4 hours), percutaneous nephrostogram.
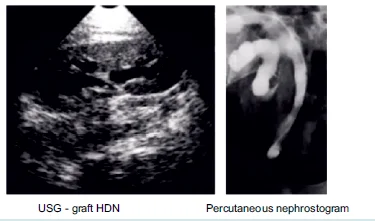
- Initial treatment: Percutaneous Transluminal Dilatation (PTD).Success rate is 90%. Best results - fresh surgical strictures. Internal or external stent placement. 10-Fr DJ stents for 10 days. <3 cm in length. Percutaneous balloon dilatation, antegrade flexible ureteroscopy and Holmium laser incision. Treat late stricture recurrence and >3 cm in length. Surgical reconstruction
- Strictures of the middle and upper ureter: Ischemic or periureteral fibrosis, require surgical intervention.
Also Read: ADRENAL GLAND -Breast and Endocrine

Prophylactic Ureteral Stents
- Can reduce the incidence of ureteral leaks and early ureteral stenosis. Would be unnecessary in 95% of patients. Danger of a forgotten stent turning up calcified later. Magnus and Haag performed a meta-analysis of 49 published studies. Significant reduction in ureteric complications with stents. Wilson and colleagues in a Cochrane review found RR of major urological complications with stents 0.24. Duration – 2 to 6 weeks (recent trend is removing the stent at 2 weeks because it minimizes the risk of infection)
Post Transplant Hematuria
- Mild hematuria: Common in first 12-24 hours. Resolves spontaneously. Extensive hematuria: Retained blood clots urinary tract obstruction, continuous bladder irrigation (to prevent clot formation), cytoscopic clot evacuation. Cauterize the bleeder-(usually distal tip of the transplanted ureter)
Erectile Dysfunction
- May occur because of side effects from immunosuppression. sed cavernosal blood supply by renal arterial anastomosis. In Sirolimus-treated men there is increased FSH and LH, decreased testosterone. Sildenafil – safe treatment. Increased GFR and doesn't alter drug levels. Intracavernosal Injections (ICIs) – Increased risk of infection. Penile prosthesis criteria- Stable graft function without a rejection crisis for 6 months. Low doses of maintenance immunosuppressants. Low probability of device malfunction. No intra-abdominal components. Prophylactic antibiotic therapy (parenteral, intraurethral, and wound irrigation) and postoperative oral antibiotics for 2 weeks.
Stone Disease
- After renal transplant there is Increased risk of stone disease, because persistent hyperparathyroidism in 38% - 77% patients. Sudden deterioration of renal function, no colic. Diagnosis: USG, RDS, antegrade pyelography. PCN placement for ureteral obstruction- Low pressure drainage, Antegrade dye study. Renal stones- PCNL (Percutaneous Nephrolithotomy) for >20 mm stones, SWL (Shockwave Lithotripsy) or antegrade/ retrograde URS for stones <15 mm. Bladder stones – Cystoscopic Lithotripsy
Also Read: Head Injury : Introduction, Fractures of Brain, Management of Fractures
Peritransplant Fluid Collections
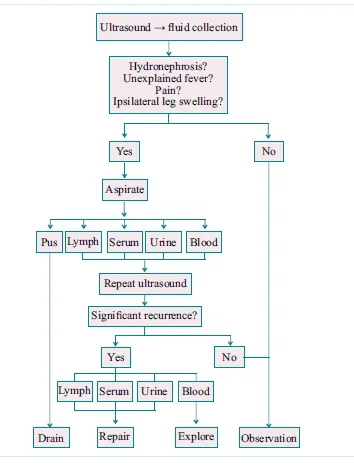
- Can occur in up to 50% of patients. Urinomas, hematomas, lymphoceles and abscesses. Immediate post-op period- Crescentic peri transplant collections are common, Document the size. Growing collections- urine leaks, abscesses or vascular injury.
Hematomas
- Usually small and resolve spontaneously. Postoperative/ trauma/ biopsy. Acute hematomas – echogenic/ high attenuating. Needle aspiration – rule out abscess.

Lymphoceles
- Incidence – 0.6 to 18%. Iliac vessel dissection, Inadequate ligation of lymphatics. Usually occur >2 weeks post transplant. Mass effect and compression of ureter/ iliac vein. Ultrasound and percutaneous aspiration for diagnosis.
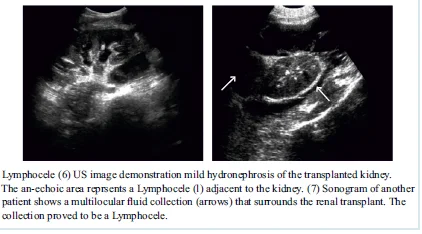
- Asymptomatic and <3 cm – resolve spontaneously. Symptomatic: Percutaneous drainage and sclerotherapy, Laparoscopic or open peritoneal window. Sclerotherapy agents: Provide iodine (Betadine), tetracycline, or fibrin glue. Marsupialization – kidney becomes intraperitoneal
Abscesses
- May be present within the first few weeks of renal transplant. Pyelonephritis or bacterial seeding of fluid collection. Fever of unknown origin, pain, or pressure symptoms. Any echogenicity within a dilated collecting system is clinically significant. Highly echogenic, weakly shadowing masses in PCS- Fungus balls. USG/ CT guided percutaneous drainage + systemic antibiotics.
Also Read: Congenital Anomalies of the Kidneys and Urinary Tract
Vascular Complications
Renal Artery Stenosis
- Pre-anastomotic – in atherosclerotic donor vessel, Anastomotic – perfusion injury, faulty technique or reaction to suture material. Post-anastomotic – rejection, turbulent flow, or arterial twisting, kinking, or compression. End-to-end anastomosis – 3 times greater risk, Suspicion – refractory HTN, audible bruit, HTN with graft dysfunction. Color Doppler USG: Frequency shifts greater than 7.5 KHz. Velocity gradient more than 2:1. MR angioplasty: No contrast required. Management options: Percutaneous transluminal angioplasty with stent. Surgical correction – high morbidity
Infarction
- Renal artery thrombosis – focal/ diffuse infarcts. Hyperacute rejection, anastomotic occlusion, arterial kinking or intimal flap. Vasculitis – small segmental infarcts. Presentation – anuria and tenderness over the graft.
AV Fistulas And Pseudoaneurysms
- Following percutaneous biopsy for suspected graft rejection. Gross hematuria – 5%-7% of biopsies, self limiting mostly. USG Doppler – localized areas of disorganized color outside the confines of normal vessel. AVF – abnormal high-velocity turbulent flow isolated to a single segmental or interlobar artery and paired vein. Feeding artery - high velocity low resistance waveform. Draining vein – arterialization. Pseudoaneurysms – appear as simple or complex renal cyst- highly vascular intracystic flow. Conservative management initially- Most resolve spontaneously. Early intervention: Progressive enlargement, Unusual size (>2 cm). Selective trans-vascular catheterization: Large AVM - steel coils, peripheral small AVM and pseudoaneurysms- microcatheter/ detachable balloon superselective catheterization, gelfoam can be used
Renal Vein Thrombosis
- Usually first postoperative week. Presentation – abrupt cessation of urinary function and swelling and tenderness over the graft. Risk factors: Hypovolemia, venous compression from a peri transplant fluid collection, dysfunctional anastomosis and slow flow. Silent iliac artery compression syndrome - left lower quadrant. USG: enlarged kidney, venous flow reduced or absent, increased resistance on the arterial side, reversed diastolic flow. MR venography – confirmatory. Management – Transplant re-exploration. Early recognition – thrombectomy may salvage allograft. Graft infarction – transport nephrectomy, Prevent secondary infection.
Also Read: Prune Belly Syndrome (Eagle Belly Syndrome)
Transplant Rejection
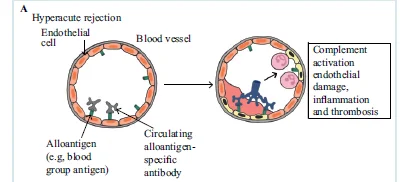
- Hyperacute Rejection
- Untreatable but universally preventable- Lymphocytotoxic crossmatch assay. Mediated by donor specific antibodies-Blood group antigens, prior transplantation, transfusion or pregnancy
Complement-mediated lysis – endothelial cell activation - procoagulant state - immediate graft thrombosis.
2. Acute Rejection
- Can be reversed once established. T-cell mediated rejection (TCMR) – lymphocytic infiltration. Antibody mediated rejection (AMR) – donor specific alloantibodies. First 6 months after transplantation. Direct and indirect alloresponse pathways.
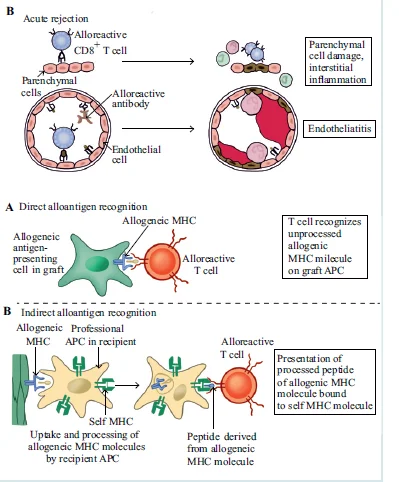
- Adequate biopsy: At least 10 glomeruli and two small arteries. Stained with hematoxylin-eosin (HE), periodic acid-Schiff stain (PAS) or silver, and trichrome stains. Two separate cores obtained – patchy distribution. Banff Working Classification of Renal Allograft Pathology-Histologic definition of rejection. Indirect marker of antibody-mediated injury-Complement (C4d) deposition. Bulk of current immunosuppressive agents- Directed at T-cell response. Prompt recognition of acute rejection is essential. Unexplained graft dysfunction- Prompt biopsy. Evaluation for lymphocytic infiltration, antibody deposition, parenchymal necrosis. Prevention strategy: Corticosteroids, Antiproliferative agents – Azathioprine, MMF. Calcineurin inhibitors – Cyclosporine, Tacrolimus. Lymphocyte Depletion agents – ATG, OKT3, anti IL-2 Ab
Management of Acute Cellular Rejection (ACR)
- First rejection – Steroids – Prednisolone 120 - 250 mg OD or Methylprednisolone for 3-5 days. Thyroglobulin or OKT-3 antibody – More severe vascular rejection. Recurrent – Steroids – not more than 2 courses, mild recurrences and separated by several weeks. Depleting Antibodies – Not fulfilling above criteria. Refractory – Add depleting antibodies. Late – 3-4 months post transplant,steroid pulse therapy, depleting antibody
Management of Antibody mediated rejection
- High dose IVIG (2 mg/Kg IV)- Plasmapheresis added to IVIG regimen. Every alternate days, until donor specific antibodies are reduced. Rituximab (anti - CD20)- epletion of antibodies producing B cells
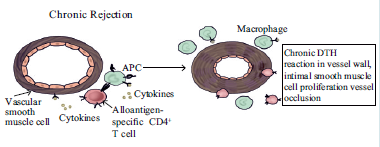
Chronic Rejection
- Most common type of transplant rejection happens in every transplant patient sooner or later. Combination of immune and non-immune effects. Interstitial fibrosis and tubular atrophy (IF- TA) or chronic allograft nephropathy. Parenchymal replacement by fibrous tissue. Prior rejection episodes – cumulative injury. Chronic inflammation.
Neoplasms
- Since the patient is on prolonged immunosuppression, hence there is 100 times more risk of neoplasm development. Prevalence – 6%. Skin malignancies and lymphoma mostly. No increase in the incidence of prostate cancer. H/o haemodialysis for ESRD – RCC risk . H/o cyclophosphamide exposure – urothelial malignancies. Gross hematuria – evaluate all present kidneys and ureters- USG/CT, Cystoscopy and RGP. Uses BCG therapy with caution for superficial masses
Post-Transplantation Lymphoproliferative Disorder
- Impaired immune surveillance and oncogenic effects of immunosuppressive therapy. Association with Epstein Barr virus. PTLD complicates 8% of transplantations. Diagnosed at a median of 80 months after transplantation. The liver, brain, and lung are common sites. Polymorphic collections of B cells- indistinguishable from Non-Hodgkin lymphoma
Infectious Complications
- Fungi such as Candida, Pneumocystis, Aspergillus, and cryptococcus. Treatment: Nystatin suspension for 1 to 3 months and Clotrimazole lozenges. Bacteria including Listeria monocytogenes, Nocardia, and Toxoplasmosis. Treatment: Clotrimazole for 3 months. Viruses such as CMV (most common viral infection), EBV, Polyomavirus, Hepatitis virus and Herpes virus. Viral infection is the most common infection overall in the transplant patients. Treatment: Valacyclovir for 3 months. Most common type of infection within the first month of transplant – Bacterial. Most common type of infection within the 6 months of transplantation – Virus.
CMV Infection
- Most important pathogen in clinical transplantation. Usually occurs 30 to 50 days after transplantation. Clinical features: Non specific signs and symptoms: Fever; Malaise; Arthralgia; Thrombocytopenia, Interstitial Pneumonia, Enterocolitis, Disseminated Disease. Diagnosis: Biopsy with histological evidence and culture. Treatment: IV Gancyclovir
BK Virus
- Polyoma virus family. Associated with nephropathy – typically occurs 1 to 4 months after transplantation. sed levels of BK virus replication Detected by PCR in blood and urine Predictive of pathology in renal transplantation. Urinary excretion of BK virus (BK uremia) associated with development of – Ureteric strictures, Nephropathy, Generalized Vasculopathy. Treatment: Early detection and reduction of immunosuppressants Reduces graft loss from 90% to 10%.
Cardiovascular Complications
- IHD accounts for up to 53% of deaths. CVD risk-More than the general population. Lower than patients on deceased donor waiting list. Measure to reduce the risk- Screening for IHD before transplantation, Perioperative blockade, Aspirin Prophylaxis, Cigarette Abstinence, Aggressive management of hypertension, Statins for patients with raised LDL levels, Glycemic control
Also Read: RENAL STONES - Etiology, Investigation and Management
Neurological Complications
Immediate
- CNS dysfunction: Hypoxic ischemic insult and perioperative sedation, Electrolyte imbalance., Rejection Encephalopathy – acute graft rejection in young patients, Hypertensive Encephalopathy, Central Pontine Myelinolysis
- PNS dysfunction: Femoral Neuropathy, Lumbosacral Plexopathy, Ulnar Neuropathy
Subacute
- CNS dysfunction: Cyclosporine, Tacrolimus – tremors, paresthesias., Steroids – mood alteration, psychosis.
- PNS dysfunction: Cyclosporine – limb paresthesias, Tacrolimus – demyelinating peripheral neuropathy, Steroids –myopathy, Guillain-Barre Syndrome – CMV related
Chronic
- Meningitis – Atypical presentation, Encephalitis, Cerebral abscesses – fungal, Progressive dementia – Progressive multifocal leukoencephalopathy, Ischemic Stroke.
Hope you found this blog helpful for your NEET SS Surgery Urology Preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Early Graft Dysfunction
Urologic Complications
Urine Leaks And Urinomas
Ureteral Obstruction
Prophylactic Ureteral Stents
Post Transplant Hematuria
Erectile Dysfunction
Stone Disease
Peritransplant Fluid Collections
Hematomas
Lymphoceles
Abscesses
Vascular Complications
Renal Artery Stenosis
Infarction
AV Fistulas And Pseudoaneurysms
Renal Vein Thrombosis
Transplant Rejection
Management of Acute Cellular Rejection (ACR)
Management of Antibody mediated rejection
Chronic Rejection
Neoplasms
Post-Transplantation Lymphoproliferative Disorder
Infectious Complications
CMV Infection
BK Virus
Cardiovascular Complications
Neurological Complications
Immediate
Subacute
Chronic
Top searching words
The most popular search terms used by aspirants
- NEET SS Surgery Urology