Urological Trauma And Indications Of Radiological Assessment
Dec 14, 2023

An injury to the urinary tract or reproductive organs. Upper urinary tract- Renal , Ureteric and Lower urinary tract- Bladder, Urethra, Genitalia.
Upper Urinary Tract
Renal Trauma
Renal injuries are the most common, around 10% of trauma cases involve the genitourinary tract trauma. Blunt injury is much more common compared to penetrating injury. Most of these renal injuries are self-limiting. If the patient is hemodynamically stable, management is conservative and those who are unstable then need to explore the patients for surgery.
Classification
Blunt injuries account for 10% of renal injuries. Penetrating injuries account for 70% of the renal injuries.
When to Suspect Major Renal Injuries?
Gross hematuria - It does not correlate with the severity of injury. Microscopic hematuria with shock. Microscopic hematuria following in children. Patients with penetrating renal injury to the flanks.

Scenario In Er
Hemodynamically Unstable
Those are subjected to focused assessment with sonography for trauma (FAST). If it is positive immediately taken to the exploratory laparotomy. On exploratory laparotomy, Peri renal hematoma is discovered. During the surgery, a single-shot intravenous pyelogram (IVP) at 10 minutes to assess the contralateral kidney.
Hemodynamically Stable
Directly subjected for contrast-enhanced computed tomography (CE-CT) which indicate the grade of injury
Indications of Radiological Assessment
Penetrating injury to the flank. Gross hematuria. Shock in combination with microscopic hematuria. Children with microscopic hematuria (Kidney is lower and less protected).
Grading of Renal Injury
Grade I
Non-enlarging Subcapsular hematoma. No parenchymal laceration.

Grade II
Superficial laceration <1.0 cm laceration. Collecting system not involved. No extravasation of urine. Non-expanding perineal hematoma confined to the retroperitoneum.

Grade III
>1.0 cm laceration. No extension into renal pelvis/collecting system. No evidence of extravasation of urine. Non-expanding hematoma.

Grade IV
Laceration extending into renal pelvis or urinary extravasation. Expanding sub capsular hematoma compressing the kidney. Segmental infarction without associated laceration. Injury to main renal artery or vein with confined hemorrhage.

Grade V
Shattered kidney. Avulsion of renal hilum: Devascularization of kidney due to hilar injury. Ureteropelvic avulsion. Complete laceration or thrombosis of the main renal artery or vein.

Grade 1, 2 and 3- hemodynamically stable conservative management. Grade 4 and 5- hemodynamically stable conservative management. But have a higher chance for conservative management failure ultimately leading to surgical care.


Absolute Indication For Intervention
Hemodynamic instability with shock. Expanding/pulsatile renal hematoma (usually indicating renal artery avulsion). Suspected renal pedicle avulsion (Grade-5). Ureteropelvic junction disruption- Partial Ureteropelvic/ ureteric injury- DJ stent is passed. Complete Ureteropelvic junction disruption- Surgery.
URINOMA
Extravasation of urine due to grade 4 injury or Partial Ureteropelvic injury confined to a particular place by the fascial planes. Treatment: Systemic antibiotics. If persists for more than 10 days- DJ stenting. DJ stent is a hollow tube placed between the renal pelvis and bladder. Percutaneous nephrostomy or Pelvic elisa drainage is the last resort.
Also Read: IMMUNOSUPPRESSION DRUGS IN RENAL TRANSPLANT
Ureteric Trauma
Q. Most Common Cause of Ureteric Rupture?
- Hysterectomy
- Ureteroscopy
- Trauma
- Abdominal perineal resection
The most common cause of Ureteric trauma is abdominal or vaginal hysterectomy. Pre-emptive ureteric catheterization used to identify ureter during the surgery and also it helps to reduce the ureter injury.
Ureter Injury Diagnosed During Intra-Operation
If ureteric injury is diagnosed intra operatively, if the patient is hemodynamically stable then recommended for primary repair. If unstable, may perform damage control – deliberate ligation of proximal ureter and insert proximal percutaneous nephrostomy.
Ureteric injury Not Diagnosed During Operation
Silent atrophy of kidney – without any symptoms it can stop function . Patients feel the symptoms includes flank pain, fever, pyonephrosis due to the injury . Fistula formation via abdomen or vagina.
Management
Treatment depends on the extent and location of ureteral trauma. No loss of length of ureter-Spatulation and ENE-TO-END anastomosis without tension.
- Little loss of length- Early stage managed non-surgical with ureteral stenting.
- Mobilize kidney.
- Psoas Hitch- Contralateral pedicle is ligated and the bladder is anastomosed with ureter on the deficient side. The bladder is then attached to the Psoas tendon to keep it in place.
- Boari operation - It will help us to gain the length.
- Marked loss of length- Transuretero ureterostomy- Injured ureter is anastomosed with the normal one.
- Disadvantage- Unilateral injury can be converted to B/L injury. Contraindications- Inadequate length, active disease, Recurrent stone formation.
- Interposition of isolated bowel loop or mobile appendix- If it all there is a long length absence, can take a bowl segment we can convert into the tubular form and fill the gap or we can perform.
- Nephrectomy- Resect the kidney and bring it to the pelvis, directly connect to the bladder.
Lower Urinary Tract
Bladder Injury
Urinary bladder is mostly extra-peritoneal but the superior and lateral border of the urinary bladder is bordered by the peritoneal cavity. So, this is the reason bladder rupture can be either Extraperitoneal rupture and Intraperitoneal rupture. Extra-peritoneal rupture is more common than intra-peritoneal rupture. Common findings of extra- and intra-peritoneal rupture. No urge to pass urine. On abdominal examination no palpable bladder.
Q. A patient came to the ER after RTA. Patient has no urge to pass urine for the last 24 hrs. Patient is hemodynamically stable. Abdominal examination of this patient is normal. On workup , the patient has a pelvic fracture. What is the diagnosis?
A. Extraperitoneal Bladder rupture.
B. Intraperitoneal Bladder rupture.
C. Anterior urethral injury
D. Posterior urethral injury
Q. Most common cause of bladder rupture?
A. Blunt abdominal trauma
B. Penetrating abdominal trauma
C. Cystoscopy
D. Obstetric and Gynecological surgery
Differences
Extra-peritoneal rupture of bladder Intra-peritoneal rupture of bladder Pelvic fracture is associated with most of the cases. Occurs after the blow in the suprapubic region when patient has full bladder. It is associated with proximal urethral injury. It is not associated with urethral injury. It leads to deep perineal hematoma. It leads to peritonitis. Cystogram Cystogram Treatment is Foley’s insertion and it is to be kept for 7 days Treatment is a laparotomy + Repair of bladder + suprapubic catheter (SPC) placement for 7-14 days.

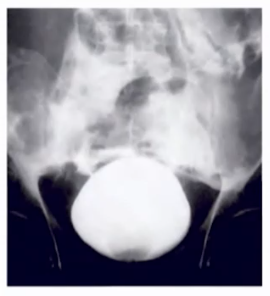
Flame shaped extravasation of contrast- Seen Extraperitoneal rupture of bladder.

Molar tooth sign of CT scan- Seen Extraperitoneal rupture of bladder.
Management
Extra peritoneal bladder rupture management
- Patients can be managed conservatively with a large 22 Fr preferred Foley’s catheter, pass it through urethra which decompresses the bladder and heal over the period of 14 days. If no healing after 14 days, undergo surgery. Other indications for surgery: Intra-abdominal injuries, Bony fragment in the bladder
Intra peritoneal bladder rupture management
- There is no role for conservative management, you can go directly for surgery.
Also Read: Complications of Renal Transplant
Urethra Trauma
Q. A 26 year old male present to you in the ER when he met with an accident while going to pick his girlfriend from her dance class. Patient is hemodynamically stable with BP of 122/80 mmHg and pulse rate of 102/min. Patient is fully conscious and he narrates the entire incident. His only complaint is he is unable to pass the urine and has pain in abdomen and suprapubic region. You examine the patient and find that the patient has distension in the suprapubic region of the abdomen and has a palpable bladder. There is blood at the external meatus and per rectal examination there is a high riding prostate. X-ray reports of the patient show pelvic fraction.
1. What is the most probable diagnosis of the patient?
- Extraperitoneal bladder rupture
- Intraperitoneal bladder rupture
- Posterior urethral injury
- Anterior urethral injury
2. What is the next line of management of this patient?
a. Suprapubic catheterization
b. Single attempt of urethral catheterization
c. Retrograde urethrogram
d. CT scan abdomen and pelvis
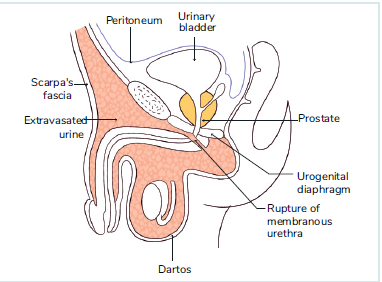
- If the patient is diagnosed with blood at meatus and inability to pass the urine. Do not try to catheterize the patient because if it is at all urethral injury it may be severe. First need to confirm urethral injury is present or not so perform Retrograde Urethrogram (RGU) - if extravasation of the dye is present, confirms the urethral injury presence. If the extravasation of the dye is not present i.e., dye reaching upto the bladder, indicates absence of urethral injury. Further, need to confirm it is in anterior or posterior urethral injury by doing SPC (supra pubic catheterization). If the extravasation of the dye is not present i.e., dye reaching upto the bladder, indicates absence of urethral injury. Then may be due to small contusion in the urethra the patient is unable to pass urine. In this scenario, a Catheter is passed and kept for 24-36 hours then we can remove it.

Common Finding In Anterior And Posterior Urethral Injury
Urge to pass the urine but unable to pass it. Palpable bladder
Differences
| Posterior urethral injury | Anterior urethral injury |
| Associated with pelvic fracture | Associated with straddle injury |
| Leads to deep perineal hematoma | Leads to superficial perineal hematoma |
| Prostate is high riding | Prostate is at a normal position |
| Associated with extra peritoneal bladder rupture | Not associated with bladder rupture |
 |
Straddle injury
When the urethra is compressed between the pubic symphysis and the rod of the bicycle.
Anterior Urethral Injury:
Retrograde urethrogram showing extravasation of urine.

Management
As patient has distended bladder and a confirmed urethral injury, do not try to catheterize the patient. Do a Supra Pubic Catheterization and send the patient home. Patient has a follow up visit after 6 week. Repeat RGU. Urethral injury resolved without any residual effects. Patient has- Developed Urethral Stricture, Treat Urethral Stricture.
Penile Fracture
- A 38-year-old man has been brought to ER at 2 AM with the main complaint of sudden onset severe pain in the penis. During sexual intercourse 1 hour ago, he heard a cracking sound followed by pain and rapid loss of penile erection. He has not been able to pass urine after the incidence and pain increases when he tries to pass the urine. On examination of the penis you see that penis is swollen and ecchymotic. You stabilize the patient by giving adequate analgesia. What is the next step in the management after this?
- Splinting of penis with cold compression
- Reassurance
- Colour doppler study
- Retrograde urethrogram
- Placement of SPC
- Tunica albuginea is covering the two corpora cavernosa and the Buck's fascia covering the corpora spongiosum and both the corpora cavernosa.

- When peris is in the erect state due to bending of penis, Rupture of corpora cavenosa due to tear in tunica albuginea. Most of the patients hear an audible snapping sound with loss of penile erection and bending of penis at the fracture site and formation of the hematoma. It is mostly a clinical diagnosis and it is a surgical emergency
Eggplant Deformity
Characteristics of penile fracture. Indicates intact Buck's fascia.

Q. After RTA, a young male came to the ER, the patient was hemodynamically unstable so the patient was taken up for exploratory laparotomy. During the operation you found a perirenal hematoma, what is the next step in the management of this patient?
A. Nephrectomy
B. Open Gerota’s fascia and explore proximal renal vessels
C. Perform retrograde pyelography
D. Single shot IVP
Q. After RTA, a young male presented with non-pulsatile retroperitoneal hematoma. On table IVU was done. Right kidney was not visualized. Left kidney showed immediate excretion of dye. What is the next step in management?
A. Nephrectomy
B. Open Gerota’s fascia and explore proximal renal vessels
C. Perform retrograde pyelography
D. Perform on table angiography
Also Read: Prune Belly Syndrome (Eagle Belly Syndrome)
If you are preparing for NEET-SS 2024 and ahead, check out SS ELITE Plan (Version 3.0) and what makes it the perfect study resource for your super speciality preparation.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Upper Urinary Tract
Renal Trauma
Classification
When to Suspect Major Renal Injuries?
Scenario In Er
Hemodynamically Unstable
Hemodynamically Stable
Indications of Radiological Assessment
Grading of Renal Injury
Grade I
Grade II
Grade III
Grade IV
Grade V
Absolute Indication For Intervention
URINOMA
Ureteric Trauma
Q. Most Common Cause of Ureteric Rupture?
Ureter Injury Diagnosed During Intra-Operation
Ureteric injury Not Diagnosed During Operation
Management
Lower Urinary Tract
Bladder Injury
Differences
Management
Extra peritoneal bladder rupture management
Intra peritoneal bladder rupture management
Urethra Trauma
Common Finding In Anterior And Posterior Urethral Injury
Straddle injury
Anterior Urethral Injury:
Management
Penile Fracture
Eggplant Deformity
Top searching words
The most popular search terms used by aspirants
- NEET SS Surgery Urology