Pancreatitis: Acute And Chronic Pancreatitis
Jun 29, 2023
Pancreatitis is the medical term for pancreatic inflammation. The pancreas is a long, flat gland that resides in the upper belly, just below the stomach. The pancreas produces enzymes that aid in digestion as well as hormones that help regulate how your body uses glucose (sugar).
There are two types of pancreatitis acute and chronic.
Read this blog further to get a quick overview of this important topic ACUTE AND CHRONIC PANCREATITIS for SURGERY to ace your NEET PG exam preparation.

Acute Pancreatitis
Acute pancreatitis is a short-term condition. It happens when your pancreas is attempting to recover from a little, transient injury. The majority of people with acute pancreatitis will recover completely in a few days with supportive care, including rest, water, and painkillers. However, a particularly severe instance of acute pancreatitis can lead to serious health problems, some of which are potentially fatal.
Causes of Acute Pancreatitis
- The most common cause is Gall stones
- Other Causes
- Blunt trauma
- ERCP (Endoscopic Retrograde Cholangiopancreatography)
- Hypertriglyceridemia
- Hyperparathyroidism
- Hypercalcemia
- Carcinoma pancreas
- Cystic fibrosis
- Viral Infections
- C – Cytomegalovirus, COX-Sackie virus
- M - Mumps
- E - Echo Virus
- Drugs Having Definite Association with Acute Pancreatitis
- M - 6 – Mercaptopurine
- A - Azathioprine
- D - Deoxy inosine
- C - Cytarabine
- A - Aminosalicylic Acid
- T - Tetracycline
- P - Pentamidine
- E - Estrogen
- T - Trimethoprim-Sulfamethoxazole
- T - Thiazide
- V - Valproate
- F - Furosemide
- M - Metronidazole
- Drugs Having Possible Association with Acute Pancreatitis: L-Asparaginase and Acetaminophen.
Pathophysiology
There is Abnormal intra-pancreatic activation of Pancreatic enzymes. These pancreatic enzymes have lipase which digests the fat of greater omentum. Fat is converted to fatty acid and glycerol. Fatty acids combine with calcium and form chalky white deposits-Saponification leading to Hypocalcemia.
It is mild and self-limited in the majority of cases. Mild Acute pancreatitis is having less than 1% mortality. Severe Acute pancreatitis is having 10-30% mortality. Gallstones-induced pancreatitis has the best prognosis.
The most common cause of death in acute pancreatitis within 2 weeks of Hospitalization is MODS (Multi Organ Dysfunction Syndrome) and after 2 weeks of hospitalization is Sepsis. The initial sign of MODS (Multi Organ Dysfunction Syndrome) is Impaired lung function (ARDS).
Symptoms of Acute Pancreatitis
Below are mentioned some of the symptoms of acute pancreatitis:
- Pain in the Epigastrium, radiating to the left side of the back and partially relieved by sitting or bending forward.
- Due to Paralytic Ileus there is Nausea, Vomiting, and Abdominal distention
- Signs of Paralytic Ileus in X-ray abdomen can be seen as:
- Gasless abdomen
- Ground glass appearance
- Sentinel loop sign – when it involves jejunum
- Colon cut-off sign – when it involves the colon

- It is associated with left-sided pleural effusion
- There is a retroperitoneal bleed into the facial planes which can be manifested by following signs:
- Cullen Sign - Ecchymosis around the umbilicus
- Grey Turner Sign - Ecchymosis around the flank
- Fox Sign - Ecchymosis around the inguinal region

Diagnosis of Acute Pancreatitis
The diagnosis of acute pancreatitis can be made with the help of some of the investigations and as it has a sudden onset the history given by patient can also help us to diagnose acute pancreatitis.
The investigation of choice is CECT (Reserved for complication; the Best time is after 72 hrs.). Diagnosis is usually made by clinical findings and laboratory Investigation. Laboratory investigations include:
- Amylase (not very specific)- It is Raised in non-pancreatic causes and there is no correlation between the level of amylase and severity of AP
- Lipase (More specific)
CECT is the Investigation of choice for the diagnosis of most of the retroperitoneal organs.

Treatment of Acute Pancreatitis
- Fluid resuscitation – The fluid of choice is Ringer lactate
- Oxygen supplementation is provided
- Analgesics
- NSAIDS → Metamizole
- OPOIDS → Buprenorphine
- Nutrition: Enteral Nutrition is preferred over TPN (Total parenteral nutrition) due to complications
- Indication for TPN (Total parenteral nutrition) is
- Shock
- Severe Acute Pancreatitis
- Prophylactic antibiotics should not be given because acute pancreatitis is side effects most of them
Assessment of Severity in Acute Pancreatitis
- RANSON’S score
- Modified Glasgow score {If the score is more than or equal to 3 it indicates Severe Acute Pancreatitis}
- BISAP Score
- Q-SOFA
- APACE – II → if Score ≥ 8 in severe acute pancreatitis
- CT Severity index: Components are Balthazar CT grading with Necrosis Score.
- CRP ≥ 130 mg/ml
- Ransons’s Prognostic Criteria (For Non-Gall Stone Induced Pancreatitis)
| At the Time of Admission | After 48 Hours |
| Age > 55 years | Fall in Hematocrit > 10 points |
| WBC count > 16,000/mm3 | BUN Elevation > 5mg/dL |
| RBS > 200 mg/dl | Serum Calcium < 8 mg/dL |
| LBH > 350 IU/L | Base deficit > 4 mEq/L |
| AST > 250 U/L | Arterial PO2< 60 mm Hg |
| Fluid Sequestration > 6 L. |
- Out of 11 if ≥ 3 present then it is suggestive of “Severe Acute Pancreatitis”
- The minimum time for complete Evaluation is 48 hrs.
2. BISAP Score (Bed Site Index for Severity of Acute Pancreatitis)
- B → BUN > 25 mg/dL
- I → Impaired Mental Status
- S → SIRS systemic inflammatory response syndrome (2 of 4) parameters are-
- Temperature (core) more than 38°C or <36°C
- Heart rate more than 90 beats/min
- Respiratory rate more than 20 breaths/min
- WBC count >12,000 cells/mm3 or <4000 cells/mm3 or >10% immature (band) cells in the peripheral blood smear
- A → Age more than 60 years
- P → Pleural Effusion
| If the Score 3 is suggestive of Severe Acute pancreatitis If the Score is 0-2 <2%mortality If the Score is 3-5 >15%mortality |
3. Q – SOFA (Quick Sequential Organ Failure Assessment)
- Respiratory Rate ≥ 22/min
- Systolic BP ≤ 100 mmHg
- Alteration in Mental Status
- Each has a score 1
| SCORE | MORTALITY |
| 0 | < 1% |
| 1 | 2-3% |
| ≥ 2 | ≥ 10% |
4. APACHE II → Acute Physiology and Chronic Health Evaluation – II
|
|
|
If a Score ≥ 8 is suggestive of Severe Acute pancreatitis.
Local Complications of Acute Pancreatitis According To Revised Atlanta Classification
|
Acute (< 4 weeks, no defined wall) |
Chronic (> 4 weeks, defined wall) |
|
|
Pancreatic Abscess
In this condition, there is Pus collection in the peripancreatic region
Treatment is USG or CT-guided Percutaneous aspiration with Antibiotics.
Pancreatic necrosis
Non-viable pancreatic tissue or peripancreatic fat. It is a sterile condition. The most common complication is an infection. The most common organism responsible is E. coli. Drugs with good pancreatic penetration power are carbapenems like Imipenem and Meropenem
Treatment is done by Repeated Necrosectomy or Surgical debridement with ongoing lavage
Chronic Pancreatitis
Chronic pancreatitis is a long-term, progressive condition. It keeps happening and just becomes worse over time. When your pancreas endures persistent harm or damage, it happens. Chronic pancreatitis will eventually harm the pancreas permanently, though it may take years. It is characterized by irreversible fibrosis of pancreatic parenchyma with ongoing inflammation which prevents your pancreas to work properly.
Causes of Chronic Pancreatitis
Chronic pancreatitis can have a wide range of reasons. Long-term alcohol addiction is the most frequent cause. Alcohol use is connected to instances in about 70% of cases.
When your body unintentionally targets your healthy cells and tissues, an autoimmune illness develops. Primary biliary cholangitis, a chronic liver illness connected to chronic pancreatitis, and inflammatory bowel syndrome, an infection of the digestive tract.
Additional factors include
- A constrained pancreatic duct, the tube that transports enzymes from the pancreas to the small intestine, a blockage of the pancreatic duct by either gallstones or pancreatic stones, and autoimmune illness, which happens when your body unintentionally targets your healthy cells and tissues.
- Having a hereditary condition called cystic fibrosis results in a buildup of mucus in your lungs.
- Genetics
- Hypercalcemia, or elevated blood calcium levels
- Hypertriglyceridemia is the medical term for having a high blood triglyceride level.
Symptoms of Chronic Pancreatitis
- Initially, you might not experience any symptoms. Even before you start to feel ill, your pancreas may have undergone significant changes. When symptoms appear, they could be:
- Most common symptom is Abdominal pain (generally in epigastrium)
- Characterized by Triad
- D - Diabetes Mellitus
- P - Pancreatic Calcification (calcifications present in 30-40% of cases)
- S - Steatorrhea
TIGARO Classification of Etiology of Chronic Pancreatitis
- T → Toxic – Metabolic
- I → Idiopathic
- G → Genetic
- A → Auto Immune
- R → Recurrent sever
- O→ Obstructive
Diagnosis of Chronic Pancreatitis
Changes in your pancreas are difficult to detect in blood tests in the early stages of chronic pancreatitis. In order to diagnose the condition, blood tests are often not used. The number of pancreatic enzymes in your blood might yet be assessed using them. Additionally, to evaluate kidney and liver function, blood tests may also be performed to examine blood cell counts. For a stool test to check the amount of fat, your doctor can ask you for a sample. It's possible that fatty stools indicate improper nutrient absorption by your body.
Doctors can diagnose you most accurately with imaging tests. To check for indications of inflammation, your doctor might recommend the following tests be performed on your abdomen:
- X-rays
- Ultrasounds
- CT
- MRI
- Investigation of choice is MRCP
- Gold Standard investigation is ERCP (it is Both Diagnostic and Therapeutic)
- On ERCP- It Shows alternate stricture and dilatation of pancreatic duct with pancreatic stones enclosed giving String of pearls or Chains of lakes Appearance or Beaded Appearance. Composition of stone is Calcium carbonate
- Endoscopic ultrasound – Most accurate investigation for diagnosis of minimal change in chronic pancreatitis.
- ROSEMONT criteria is based on Endoscopic ultrasound findings for the diagnosis of chronic pancreatitis.

Treatment of Chronic Pancreatitis
- For Exocrine Insufficiency – Enteric-coated Pancreatic Enzyme Supplementation is given
- For Endocrine Insufficiency – Insulin is given
- Pain - Analgesics
- NSAIDS – Metamizole
- Opioids - Buprenorphine
- If Pain is not relieved with analgesics: ERCP (Endoscopic Retrograde Cholangiopancreatography) with stenting or oblique stone removal
- If Pain not relieved with ERCP (Endoscopic Retrograde Cholangiopancreatography) and stenting: Celiac Ganglion Block
- If Pain not relieved with Celiac Ganglion Blockade: Surgery
Surgery
| Drainage Procedure | Resection Procedure |
| Puestow’s procedure Also known as LPJ (Longitudinal Pancreaticojejunostomy). Opening pancreatic duct and anastomosed with the jejunum. 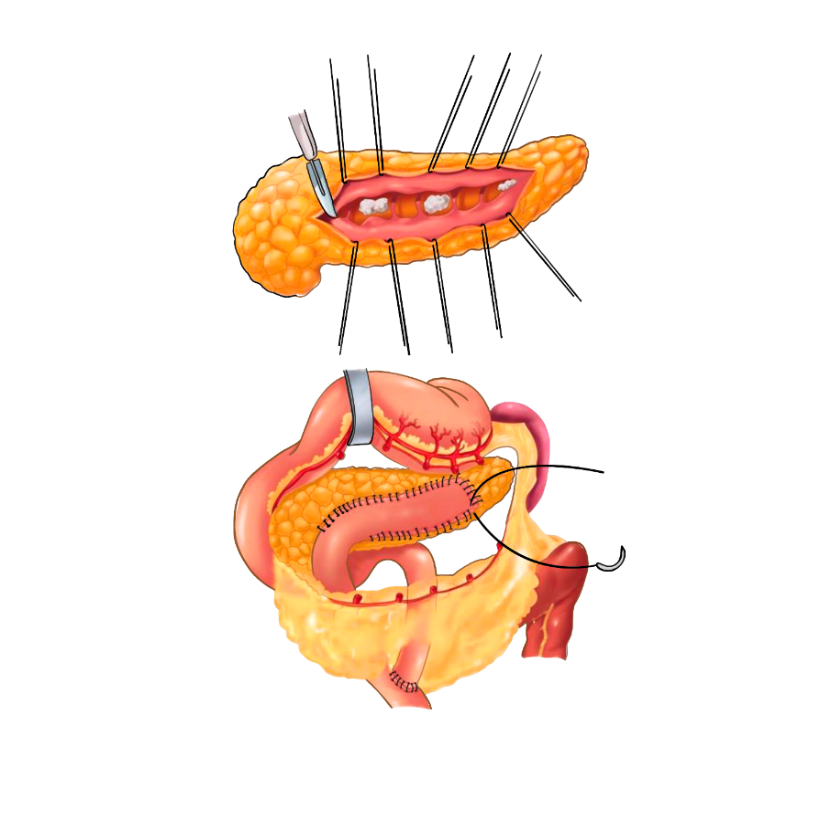 | BEGER’s procedure FREY’S procedure BEGER’S Procedure Also known as DPPHR - Duodenal preserving pancreatic head resection. After resection of the pancreatic head. The pancreatic Head anastomosed with the body with jejunum. It Has maximum Pain Relief.  FREY’S Procedure Also known as LRLPJ ( Local resection of Pancreatic head with Longitudinal Pancreatic – jejunostomy). Pancreas is excoriated along its whole length then the head is being excoriated. After that perform anastomosis along its whole length  |
To scale up your NEET PG preparation with the best-in-class video lectures, QBank, Mock Tests, and more, download the PrepLadder App!
Download PrepLadder's NEET PG preparation app for Android
Download PrepLadder's NEET PG preparation app for iOS

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Acute Pancreatitis
Causes of Acute Pancreatitis
Pathophysiology
Symptoms of Acute Pancreatitis
Diagnosis of Acute Pancreatitis
Treatment of Acute Pancreatitis
Assessment of Severity in Acute Pancreatitis
Pancreatic Abscess
Pancreatic necrosis
Chronic Pancreatitis
Causes of Chronic Pancreatitis
Symptoms of Chronic Pancreatitis
TIGARO Classification of Etiology of Chronic Pancreatitis
Diagnosis of Chronic Pancreatitis
Treatment of Chronic Pancreatitis
Top searching words
The most popular search terms used by aspirants
- NEET PG Surgery