Tetralogy of Fallot: Causes, Symptoms, and Surgical Treatment
Jun 1, 2023

The rare disorder known as tetralogy of Fallot is caused by a congenital (present at birth) combination of four heart anomalies. These structural issues with the heart allow oxygen-poor blood to seep out of the heart and into the rest of the body. Children and infants with tetralogy of Fallot generally display skin that is tinged blue because their blood does not contain enough oxygen.
Tetralogy of Fallot is frequently identified either immediately after birth or when the kid is still a newborn. Depending on the severity of the anomalies and symptoms, tetralogy of Fallot can occasionally go unnoticed until adulthood. It is the Most common congenital cyanotic heart disease in children.
Read this blog further to get a quick overview of this important topic for anatomy and ace your NEET PG exam preparation.
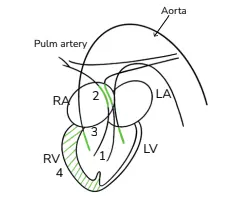
4 Components of tetralogy of fallot includes:
- Large, non restrictive Ventricular Septal defect.
- Right ventricular outflow tract obstruction (RVOT) or pulmonary stenosis (infundibular or subpulmonic>valvular)
- Overriding of aorta
- Right ventricular hypertrophy

Pathophysiology
Ventricular Septal Defect
VSDs are divided into different groups based on where they are located on the ventricular septum. The inferior aspect is where the bigger muscular septum is attached, while the superior aspect is where the smaller membranous septum is found.
Perimembranous VSD, is the most prevalent kind linked to TOF, and it is defined as a VSD that involves portions of the membrane and muscular septum. Muscular VSDs and doubly committed VSDs, which are found close to both the pulmonary and aortic valves, are additional VSDs connected to TOF.
The systolic pressures between the ventricles equalize since the VSD is often quite large. Blood shunts from the left to the right through the VSD in mild TOF because the left ventricular pressures are still higher than the right ventricle. These patients typically have cyanosis.
Pulmonary Stenosis
The location of pulmonary stenosis allows for classification. The infundibular septum (50%) is the most frequent site. Right ventricular outflow tract ("RVOT") is a word that some authors prefer, however they both essentially refer to the same structure. Additionally, valvular stenosis is seen in 10% or a mix of both 30% may be present.
Deoxygenated blood cannot flow as freely into the major pulmonary artery (PA) as a result. This forms the basis of hypoxic episodes, often known as tet spells, and may be severe enough to produce intermittent RVOT blockage ("RVOTO").
Right Ventricular Hypertrophy
The right ventricle has ventricular hypertrophy as a result of the intense pressures and it must endure to push deoxygenated blood through the RVOTO. The 'boot' sign, which often develops in pregnancy, can be observed on chest x-rays.
Overriding of Aorta
The aorta is dilated and displaced over the interventricular septum in TOF in comparison to the healthy heart. Increased blood flow via the aorta, which receives blood from both ventricles via the VSD, results in aortic dilatation. Multiple aorto-pulmonary collateral arteries (also known as "MAPCAs") may emerge in cases of severe TOF to aid in boosting pulmonary blood flow.
Timing of Presentation & Severity Will Depend on
- Degree of pulmonary stenosis
- Ductus arteriosus open or not
Clinical features
- Cyanosis(central) due to hypoxia:spo2=75-85%
- Clubbing
- Polycythemia
- Cyanotic spells
- Dyspnoea on exertion (improves on squatting)
- Heart failure is not seen in TOF, unless it is complicated by Anemia, Infective endocarditis, Myocarditis and Systemic hypertension
Age of Presentation Depends on Severity
- Mild Pulmonary stenosis leads to pink color showing sign of tetralogy of fallot
- Mild to mod.TOF- present after 1st few months of life
- Severe TOF: in this cyanosis is present even at birth
- TOF with pulmonary atresia: in this the blood goes to the lungs via ductus arteriosus(PDA) or via MAPVA (multiple aorto-pulmonary collateral arteries).
- Cyanotic spells are most common in infants with mild TOF because compensatory polycythemia not yet developed
Risk Factors for Tetralogy of Fallot
It has an unknown specific etiology, however some factors may raise the likelihood that a baby may be born with the disorder. Tetralogy of Fallot risk factors include:
- A viral infection for example rubella in pregnancy
- Pregnancy and alcohol consumption
- An inadequate diet during pregnancy
- A parent who has tetralogy of Fallot or a woman who is over 40
- Whether the infant has DiGeorge syndrome or Down syndrome

Complications of TOF
- Cerebral thrombosis: due to polycythemia & dehydration in children of less than 2 years of age.
- Cerebral abscess in more than 2 years of age
- Bacterial endocarditis
Investigations
- Chest x-ray shows Boot Shaped Heart (or) 'Cor En Sabot' Appearance with Pulmonary Oligemia
- ECG shows right ventricular hypertrophy changes
- 2D ECHO with doppler is confirmatory of tetralogy of fallot
- General examination: clubbing, central cyanosis
- On Auscultation-
Loud, Solitary S2 is heard which is caused by absence or diminished pulmonary valve closure (P2) depending on the degree of stenosis and aortic valve closure in diastole. It is Best auscultated on the upper or middle left sternal edge (LSE) is the pansystolic murmur. The murmur becomes louder and vice versa when the VSD gets small.
Ejection click is a high-pitched sound that semilunar (aortic or pulmonary) valves make when they are fully opened. Aorta dilation is the cause of clicks in TOF. Heart normally follows S1 immediately. Continuous mechanical murmur is heard Especially in TOF patients receiving prostaglandin infusions, occurs when PDA is present and there are extreme forms of TOF.
Treatment of Cyanotic Spell
1. Moist O inhalation it decreases pulmonary vascular resistance
2. Injection Sodium Bicarbonate helps to neutralize acidosis
3. Morphine
4. Ketamine increases systemic vascular resistance
5. Alpha agonists like Phenylephrine
6. Beta blockers like Propranolol decreases pulmonary infundibular spasm, used as prophylactic medicine
7. Squatting or knee chest position helps abort cyanotic spells. It increases systemic vascular resistance, decreases venous return to right side of heart
8. PRBCs transfusion
Surgical Treatment of TOF
Definitive (corrective) surgery is ventricular septal defect closure and Repair of Pulmonary stenosis
Shunt (palliative) Surgery- In this the Connection is made between pulmonary artery & aorta or its branch.
To scale up your NEET PG preparation with the best-in-class video lectures, QBank, Mock Tests and more, download the PrepLadder App!
Download PrepLadder's NEET PG preparation app for Android
Download PrepLadder's NEET PG preparation app for iOS

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Pathophysiology
Ventricular Septal Defect
Pulmonary Stenosis
Right Ventricular Hypertrophy
Overriding of Aorta
Timing of Presentation & Severity Will Depend on
Clinical features
Age of Presentation Depends on Severity
Risk Factors for Tetralogy of Fallot
Complications of TOF
Investigations
Treatment of Cyanotic Spell
Surgical Treatment of TOF
Top searching words
The most popular search terms used by aspirants
- NEET PG Anatomy