Diuretic Drugs: Classification and Uses
Jan 2, 2026


What are diuretics?
Diuretics are drugs that increase Sodium and water excretion in the urine.
Diuretics are used when sodium and water retention are more common in conditions like edema, hypertension, and congestive heart failure.
What is the basic use of diuretics?
It is used in edema when there is water and sodium retention.
Cardiac reasons: congestive heart failure, pulmonary edema.
In a head injury, cerebral edema.
Cirrhotic edema.
Kidney reasons: CKD and nephrotic syndrome.
Another condition where sodium is unwanted is in the case of hypertension.
|
|
Elimination of Sodium and Water from the Body
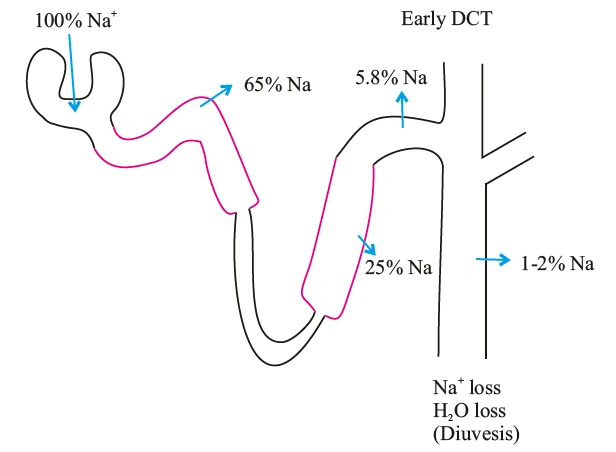
The elimination is mainly done by nephrons. 100% of sodium is filtered at the glomerulus.
In that 100%, 65% of sodium is reabsorbed into the proximal convoluted tubule. 25% of the sodium is reabsorbed in the thick ascending loop of Henle. Around 5-8% is reabsorbed in the early part of the DCT. 1 to 2% of the sodium is reabsorbed in the collecting ducts. If the reabsorption of sodium is stopped, it will go into the urine, and water will follow.
But wherever water goes, sodium will not follow. If sodium is lost, water will also be lost, and this condition is known as Diuresis. The drug that does this is called diuretics.
The Drugs that Prevent Sodium Reabsorption
The drugs that act on the proximal convoluted tubule are called carbonic anhydrase inhibitors. They inhibit the enzyme carbonic anhydrase. Their major site of action is PCT. The drugs that prevent sodium reabsorption in the thick ascending loop of Henle are called loop diuretics. Drugs that prevent sodium reabsorption into the early DCT are called thiazide diuretics.
Among these, which has more efficacy?
Carbonic anhydrase is going to inhibit sodium reabsorption with bicarbonate reabsorption. Sodium is reabsorbed along with bicarbonate, chloride, amino acids, and glucose. The sodium reabsorption is continuous with chloride reabsorption and glucose reabsorption. If a carbonic anhydrase inhibitor is used, there is a chance that sodium is getting reabsorbed in the loop of Henle.
This is why carbonic anhydrase inhibitors are mild diuretics because it is interfering with one pathway, which is sodium and bicarbonate reabsorption. Sodium is still reabsorbed along with the rest of the constituents.
The carbonic anhydrase inhibitors, loop diuretics, and thiazide diuretics are Sulfa derivatives. Patients will have allergic manifestations. These drugs tend to lose sodium when there is a loss of sodium, the aldosterone helps in the reabsorption of the sodium into the collecting duct to compensate for the sodium entry, and the potassium goes out. All three of these drugs can cause hypokalemia.
Also Read: Rapid Revision Reignite Pharmacology: Question-Answer Format
Compensation of Hypokalemia
Hypokalemia is compensated for by potassium-sparing diuretics that act at the level of the collecting ducts. These will spare the potassium and not allow it to get lost by interfering with the reabsorption of only one to two percent of sodium. These are very weak diuretics. Osmotic diuretics that can act throughout the nephron. These have high efficacy.
.jpg)
Targets of the Drugs
Carbonic Anhydrase Inhibitors
They inhibit carbonic anhydrase enzymes. The inhibition of carbonic anhydrase is a non-competitive enzyme inhibition.
- Acetazolamide
- Brinzolamide
- Dorzolamide
- Dichlorphenamide
Acetazolamide inhibits carbonic anhydrase. When it is inhibited, one will not get H+ to exchange with sodium. H+, thus, cannot combine with bicarbonate. Sodium and bicarbonate are therefore not reabsorbed. This causes a loss of sodium and bicarbonate in urine. This is responsible for the diuretic effect.
Loss of Bicarbonate in the Urine
On the loss of bicarbonate in urine, the urine will become alkaline. This increases the chance of calcium and phosphate stones. Loss of bicarbonate causes metabolic acidosis. When the
bicarbonate is lost, the proximal convoluted tubule will increase reabsorption of chloride. The patient will have hyperchloremia. This condition is called hyperchloremic metabolic acidosis.
Also Read: NEET-PG 2025 Recall Questions - Download the FREE PDF
Uses
Acetazolamide is the drug of choice for acute mountain sickness or high-altitude sickness.
When a person ascends to a high altitude, there is hypoxia, causing the patient to breathe faster and lose carbon dioxide. This will lead to respiratory alkalosis. This drug compensates for that by producing metabolic acidosis. A patient at a high altitude develops pulmonary edema, and this being a diuretic can take care of it.
Dorzolamide and brinzolamide are used for glaucoma. Dichlorphenamide has been shown to have an effect in the case of familial periodic paralysis.
Loop Diuretics (high efficacy diuretics)
The site of action of these is the thick ascending part of the loop of Henle. In that, they inhibit the transporter called Sodium Potassium 2 Chloride cotransport.
Drugs
- Furosemide: The brand name is Lasix, the drug that was lost for 6 hours.
- Torsemide: This is long-acting.
- Bumetanide: This is the most potent and is used in low doses.
- All these drugs are derived from sulfa and hence cause an allergy.
- Ethacrynic acid is a non-sulfa drug. When a person has a sulfa allergy and prefers loop diuretics, this drug can be used.
Also Read: Pharmacology Important Questions for NEET PG/FMGE 2026
Uses
Pulmonary oedema - Diuretic of choice is furosemide. Furosemide releases vasodilatory prostaglandins, which dilate the veins in the periphery. This will cause the fluid to be more in the veins and less in the lungs. This will shift the blood from pulmonary to systemic circulation. This will help the patient to breathe easily.
- Edema
- Cirrhotic edema
- CKD
- Nephrotic Syndrome
- Hypercalcemia
- Hypertension (GFR < 30ml/min). It can also be used in hypertensive emergencies
- CHF
- Acute
- Chronic
- These are high-efficacy diuretics that cause high urine and are not preferred for chronic therapy. When used for a long period, there is a chance of developing resistance, and they are only given for a shorter period.
Thiazide Diuretics
Thiazide diuretics include:
- Chlorothiazide,
- Hydrochlorothiazide.
Thiazide-like diuretics include:
- Chlorthalidone (longer acting),
- Indapamide,
- Metolazone
Thiazides are not effective in CKD patients except for metolazone, even when the GFR is 15 ml/min.
Also Read: Last 5-Year PYQs in Pharmacology for INI-CET
Uses
These are the first-choice drugs for hypertension. These are mild anti-hypertensives and can decrease the blood pressure by 5 to 10 mm/Hg.
- Edema:
- CHF
- Cirrhotic edema
- Osteoporosis: Because it will help in calcium reabsorption.
These are used to decrease renal calcium stones. If the patient is prone to renal stones again and again, then a thiazide can be used. Diabetes insipidus: both central and peripheral
Potassium Sparing Diuretics
The main site of action for these drugs is the collecting duct. Sodium enters through the epithelial sodium channel. This is potentiated by a drug called aldosterone, which acts through
the nuclear receptor. Aldosterone enters the nucleus through the aldosterone receptor. Aldosterone-induced protein is produced in the nucleus, which increases sodium reabsorption. The potassium and H+ will be thrown out.
Uses
Corrects hypokalaemia due to diuretics. Conn's syndrome or hyperaldosteronism. Resistant hypertension which is caused because aldosterone levels are very high. Cirrhotic edema, the diuretic of choice. Chronic CHF, it will decrease mortality. Spironolactone blocks the effect of aldosterone and prevents these effects. Hirsutism and PCOD patients because it has an androgenic effect blocking property.
Epithelial Sodium Channel Blockers
Uses:
Cystic fibrosis. Used in Liddle's syndrome. ENaC channels are hyperactive and will retain more and more sodium and water. Lithium-induced diabetes insipidus, in which case it is a drug of choice.
There is a channel (epithelial sodium channel) through which lithium and sodium both enter. Entering lithium decreases the activity of ADH (anti-diuretic hormone). This will lead to the patient having diabetes insipidus. Amiloride blocks the entry of lithium and thereby blocks diabetes insipidus. Hyperkalaemia and metabolic acidosis also occur in this case.
Osmotic Diuretics
These include:
- Mannitol.
- Glycerol.
- Urea.
- Isosorbide.
This acts on the tissue. When a patient is suffering from cerebral oedema. Mannitol is given; it enters the blood vessels. It is an osmotic agent and will pull the excess from the oedema water into the blood vessel. When water increases inside the blood vessels, there is a decrease in pressure in the tissue.
This causes an increase in blood volume (ECF). The volume will be carried into the heart, and the heart must work more. When the heart pumps, it reaches the nephron. It can act through the entire nephron, but its major place of action is the PCT. Since it is an osmotic agent, it will not allow water to go out of the lumen.
This will cause massive diuresis along with electrolyte abnormalities. This drug is used in cerebral oedema due to decreased blood pressure. It is used in acute congestive glaucoma.
When there is pulmonary edema, the left ventricle has failed. There is back pressure on the lung. Mannitol is not used in pulmonary edema. Because this drug increases the blood volume, an increased workload is placed on the heart. Since the left ventricle has already failed now, if it fails more and more, pulmonary edema worsens.
In case of head injury and bleeding, blood vessels inside the brain tissue are damaged, and there is bleeding. If mannitol is given to such a patient, it will leave the blood vessel,
causing more water to be drawn and the intracranial pressure to increase. If there is no active bleeding, mannitol can be used.
Uses
It is a drug of choice for cerebral edema. It is a drug of choice for acute congestive glaucoma.
It is used in poisoning so that the poison can easily be eliminated through diuresis.
It is used in impending renal failure. There is a decrease in functioning in such a case, and little urine is coming out (oliguria). Mannitol will increase blood volume and urine formation through vasodilation. More urine falls out. It increases the ECF volume, blood volume, and renal blood flow, GFR increases, and urine output increases, helping with oliguria.
Important questions and answers
Q1. What are diuretics?
They are drugs that increase the sodium and water excretion in urine.
Q2. What is the basic use of diuretics?
It is used in edema when there is water and sodium retention.
- Cardiac reasons: congestive heart failure, pulmonary edema.
- In a head injury, cerebral edema.
- Cirrhotic edema.
- Kidney reasons: CKD and nephrotic syndrome.
Another condition where sodium is unwanted is in the case of hypertension.
Q3. What is the major site of action of osmotic diuretics?
Ans: The major site of action of osmotic diuretics is the proximal convoluted tubules and the loop of Henle.
Q4. What happens to the V max and KM if it is a non-competitive inhibition?
Ans: V max decreases, and KM remains the same.
Q5. Can loop diuretics be used with NSAIDs?
Ans. When combined, vasodilatory prostaglandins will not be able to work and will not be able to provide the vasodilatory effect. That is why this combination is irrational.
Q6. How to spare the potassium?
Ans. The aldosterone receptor is blocked. The epithelial sodium channel can be blocked. This will block the sodium from entering. Potassium stays inside, leading to hyperkalaemia. H+ also stays inside, causing metabolic acidosis.
Q7. When is a loop diuretic or Thiazide Given?
Ans. Sodium enters, and potassium comes out. Because potassium is not in circulation, to compensate for that, H+ will also come out. When a loop diuretic or a thiazide is given, Hyperkalaemia occurs along with metabolic alkalosis.

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
What are diuretics?
What is the basic use of diuretics?
Elimination of Sodium and Water from the Body
The Drugs that Prevent Sodium Reabsorption
Among these, which has more efficacy?
Compensation of Hypokalemia
Targets of the Drugs
Carbonic Anhydrase Inhibitors
Loss of Bicarbonate in the Urine
Uses
Loop Diuretics (high efficacy diuretics)
Drugs
Uses
Thiazide Diuretics
Uses
Potassium Sparing Diuretics
Uses
Epithelial Sodium Channel Blockers
Osmotic Diuretics
Uses
Important questions and answers
Q1. What are diuretics?
Q2. What is the basic use of diuretics?
Q3. What is the major site of action of osmotic diuretics?
Q4. What happens to the V max and KM if it is a non-competitive inhibition?
Q5. Can loop diuretics be used with NSAIDs?
Q6. How to spare the potassium?
Q7. When is a loop diuretic or Thiazide Given?
Top searching words
The most popular search terms used by aspirants
- NEET PG Pharmacology
- NEET PG Pharmacology Preparation