Sleep Disorder : Symptoms, Causes & Treatment
Mar 29, 2023

The world of sleep disorders is a large and complex field. There are various stages of sleep, different ages when disorders of a particular kind occur, and treatments are given accordingly.
Read this blog post to know everything about sleep disorders and level up your Psychiatry preparation. We have also included a few questions towards the end.
- Sleep is made of 2 physiological states
- NREM: Non-Rapid Eye Movement.
- REM: Rapid Eye Movement.
- Once the person falls asleep, the 1st stage occurs is NREM sleep and after some time the person reaches the 1st REM. Again the person reaches NREM and then REM. The cycles alternate.
- REM Latency – time taken from the NREM to the 1st REM is known as REM Latency.
- Normally the 1st REM is reached at 90 min. There are certain conditions in which the REM is achieved earlier. There is a shortening of REM Latency.

EEG (Electroencephalogram)
- It is the recording of the electrical activity of the brain. The electrodes are placed on the scalp and the potential difference is recorded.
Frequency
- It is the number of waves that occur in a second.
- To calculate the frequency: the distance between 2 vertical lines is 1 sec and in this 1 sec the number of waves is counted. E.g., if 3 waves are seen, the frequency will be 3Hz.
Important Waves seen in EEG in Humans
Delta Waves (λ)
- Seen in deep sleep which is also known as Delta sleep.
- It is also seen in infants.
- The frequency of these waves is around 0.5-3Hz.
- The amplitude or the micro voltage of these waves is quite high. It may be ≥75µV.
- These waves are seen in slow wave sleep or deep sleep or delta sleep.
Theta Waves (θ)
- It is the transition from wakefulness to sleep.
- It is the 1st wave that is encountered in sleep.
- These are also seen in children.
- The frequency of these waves is 4-7Hz.
- These are low-voltage waves.
- They are prominently seen in the temporal and parietal regions.
Alpha Waves (α)
- Seen at rest – When the person is awake but the eyes are closed. The frequency of these waves is 8-13Hz.
- These are also low-voltage waves.
- They are seen in occipital and parieto-occipital areas.
Beta Waves (β)
- Seen in a fully awake person (eyes open).
- The frequency is higher (14-30Hz).
- These are low-voltage waves.
- They are present in the frontal and parietal areas.
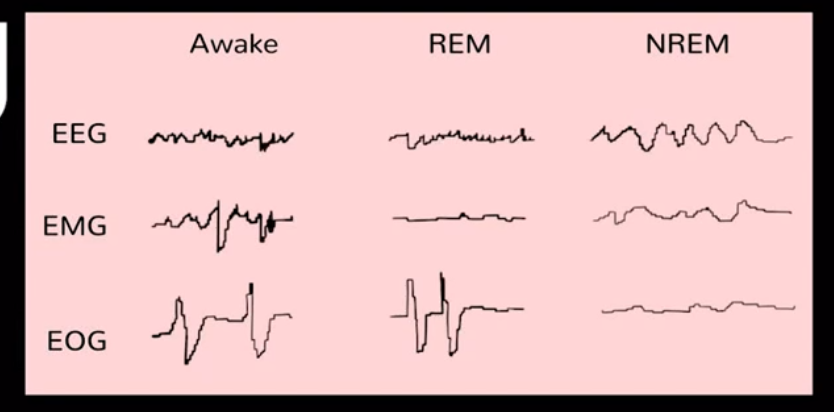
Sleep Stages
- Sleep stages are characterized by 3 parameters:
- EEG (Electroencephalogram): Measures the electrical activity of the brain.
- EOG (Electrooculogram): Measures the activity of eye movements.
- EMG (Electromyogram): Measures muscle activity.
- Sleep is scored in Epochs of 30 seconds.
Distribution of Sleep in Young Adulthood
- The normal duration of sleep is 7-9 hours. In a young adult, this may decrease.
- The duration of sleep decreases in the elderly age and increases at a young age.
- Sleep is divided into 2 stages.
- NREM
- REM
- NREM: NREM is further divided into 3 stages
- Stage 1: N1 stage
- Stage 2: N2 stage
- Stage 3 and Stage 4: Stages 3 and 4 have been combined into one stage known as the N3 stage.
- REM
- Overall, in NREM, about 75% of the time is spent in sleep and 25% is spent in REM.
- In the N1 stage, around 5% of the time is spent in sleep.
- In the N2 stage, 45% of the time is spent in sleep.
- In the N3 stage, 25% of the time is spent in sleep.
- The maximum time is spent in the N2 stage.
Various Stages of Sleep and Important Changes in EEG, EOG, AND EMG
NREM
- When the person is awake (known as stage W)
- EEG: Will show alpha waves (8-13Hz) with eyes closed.
- EOG: The eye movements and eye blinks are present.
- EMG: High tonic activity and voluntary movements are seen because the person is awake.
- When the person falls asleep and reaches the N1 stage
- EEG: There is a loss of alpha waves because the person has transitioned to sleep. There will be theta waves of 4-7Hz.
- EOG: There will be slow eye movements.
- EMG: The tonic activity decreases.
- When the person reaches the N2 stage
- EEG: There are 2 important EEG findings N2 stage:
- Sleep spindles: a burst of waves of 12-14Hz are seen.
- Presence of K complexes: these are negative sharp waves followed by positive waves.
- EOG: The EOG activity will be none.
- EMG: Muscle tonic activity will be very low.
- When the person reaches the N3 stage (Deep sleep)
- EEG: Delta waves (slow waves) will be seen. The amplitude will be high.
- EOG: The activity will be none.
- EMG: Low tonic activity is seen.
REM: Rapid Eye Movement (Paradoxical sleep)
- EEG findings
- The EEG activity is increased similarly to the awake state (beta activity) along with the return of alpha activity.
- There is a typical appearance of these waves seen which is known as Sawtooth waves or Sawtooth appearance. The appearance of these waves is Sawtooth.
- Paradoxical sleep: even though the person is sleeping the EEG shows activity similar to the awake state.
- PGO (Ponto Geniculo Occipital) spikes are also seen. These are large phasic potentials that originate from Pons (the cholinergic neurons) and go towards the lateral geniculate body and to the occipital spikes.
- EOG: Rapid eye movements are seen.
- EMG: There is tonic atonia (as if the muscle is in paralysis) with phasic twitches.
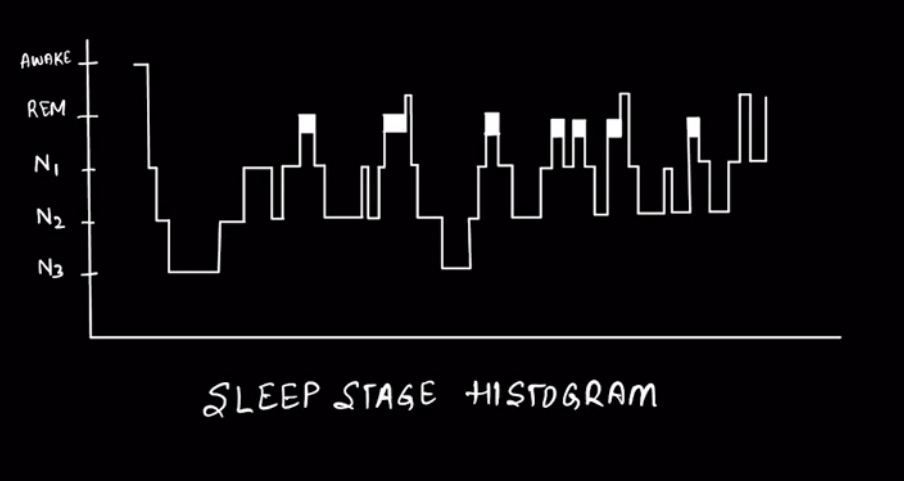
- Sleep occurs in cycles of NREM and REM.
- The total of each cycle lasts 90-110 min.
- Usually, 4-6 REM periods occur each night.

Differences Between NREM and REM
NREM
- It is known as orthodox or conventional sleep
- Brain activity & physiological activity like pulse rate, respiratory rate, and BP are lower than in the awake state.
- If there is any movement, then it is a disorder of NREM.
- Minimal variations are there in parameters such as pulse rate, respiratory rate, and BP. That is why it is known as synchronized sleep.
- There is a Pulsatile release of Gonadotropins and Growth hormones.
- Body movements are present.
- Penile erection is absent.
- Dreams are not remembered.
REM
- It is a paradoxical sleep (the person is asleep but the EEG is showing the activity of the active day).
- Brain activity and physiological activity area increased or same as in the awake state except for the muscle tone (the muscles are in the state of paralysis).
- As there are lots of variables in REM, it is known as desynchronized sleep.
- Body movements are absent.
- Penile erection is present.
- Dreams are remembered.
Also Read Psychiatry Related More Articles:
Sleep-Wake Disorders Dyssomnia
- They are characterized by abnormality of either the quantity of sleep or the quality of sleep.
- There are two dyssomnia: Insomnia and Hypersomnia.
Insomnia
- It is the difficulty in sleeping.
- The abnormalities in insomnia are:
- Initial Insomnia: Sleep initiation is difficult. It takes time to fall asleep.
- Middle Insomnia – There is difficulty in maintaining sleep. The person wakes up many times in between.
- Late Insomnia: When the person wakes up early morning (at least two hours before the usual wake-up time). Early morning awakening is one of the characteristics of depression.
- Non restorative sleep: The duration of sleep is same but the person doesn’t feel fresh in the morning due to poor quality of sleep
- Types of Insomnias
- Primary Insomnia: No cause found. Insomnia is the only symptom.
- Secondary Insomnia: Caused due to some other disorders like psychiatric disorders and depression.
- Treatment
- Pharmacotherapy
- Drugs such as Benzodiazepines, Zolpidem, and Zaleplon are helpful.
- Other sedative drugs may also be used.
- Psychotherapy
- Cognitive Behaviour Therapy (CBT) – Cognitive therapies are used to overcome misperceptions and disruptive thoughts about sleep.
- Certain behaviour techniques such as universal sleep hygiene are used to improve sleep.
- Pharmacotherapy
- Universal sleep hygiene – Certain modifiable environmental and lifestyle components are focussed on to improve. The dos and don’ts of Universal Sleep Hygiene are as follows:
- Do’s
- Maintain fixed sleeping and waking time.
- If the person feels hungry at night, eat a light snack before sleep.
- A regular exercise schedule should be maintained.
- Unwind everything one hour before sleep.
- Keep the room cool, dark, and quiet.
- Don’ts
- Taking naps.
- Eating a heavy meal before sleeping.
- Exercise before sleep.
- See the time when unable to sleep.
- Use alcohol and smoke cigarettes.
- Reading, eating, watching TV, and talking on the phone in bed.
- Do’s
Some Disorders Associated with Insomnia
- Restless Leg Syndrome (Ekbom Syndrome)
- There is an irresistible urge to move the legs when the person is at rest or while trying to fall asleep.
- There is an uncomfortable sensation in the legs such as insect crawling which gets relieved by moving or walking around.
- It can cause difficulty in sleep initiation as the patient keeps on moving the legs. It can lead to secondary insomnia.
- Uremia, Neuropathies, and Iron and Folic acid deficiencies can cause secondary RLS.
- Ferritin levels should be checked in all the patients of RLS.
- Treatment – Three Dopamine agonists have been approved by the FDA for RLS treatment.
- Pramipexole
- Ropinirole
- Rotigotine
- Periodic Limb Movement Disorder (PLMD)
- There is a sudden contraction of a group of muscles usually the leg while sleeping.
- These are primarily seen in NREM.
- They can lead to brief arousals from sleep and cause insomnia.
- A person may not be aware of these contractions because they may occur in sleep but the partners sleeping next to the person may frequently get disturbed.
- It can occur in association with folic deficiencies, renal disease, and anemia.
- Treatment – Benzodiazepines may be used which are sufficient for the treatment of PLMD.
Hypersomnia
- There is excessive sleepiness.
- There may be prolonged sleep episodes.
- There may be excessive daytime sleepiness.
- Types
- Primary Hypersomnia – no cause found.
- Secondary Hypersomnia – due to some other disorders
Also Read: Nymphomania: Causes, Symptoms, Risk Factors, Diagnosis, Treatment
Disorders Associated with Hypersomnia
- Narcolepsy
- The intrusion of REM sleep into wakefulness.
- It usually begins in the second decade (between 10 and 20 years).
- Symptoms – Tetrad of symptoms:
- Sleep attacks
- This is the most common symptom.
- There is a strong urge for excessive daytime sleepiness.
- Cataplexy
- There is a sudden loss of muscle tone. The person is standing and suddenly may fall (the person is awake).
- It is triggered by emotional outbursts commonly with laughter.
- Sleep Paralysis
- The person wakes up but is unable to move the body.
- Hypnagogic and Hypnopompic hallucinations
- These hallucinations occur at a specific time.
- These can be auditory, or visual.
- Hypnagogic occurs when the person is going to sleep. The person falls asleep and experiences some hallucinations.
- Hypnopompic occurs when the person comes out of sleep.
- Sleep attacks
- Reduced REM latency.
- Cause
- Deficiency of Hypocretin (Orexin) neurotransmitter of the hypothalamus in the brain which is required for alertness.
- There is a strong association with human leukocyte antigens Class II (specially HLADR2 and HLADQB 06: 02).
- It is believed that it is an autoimmune process that leads to the destruction orexin producing neurons which lead to the development of Narcolepsy.
- Types
- Type-1 Narcolepsy
- The patient has Narcolepsy with Cataplexy.
- Low levels of Hypocretin are seen.
- Type-2 Narcolepsy
- The patient has Narcolepsy without Cataplexy.
- Hypocretin levels are normal. It can be induced by traumatic brain injury damaging orexin-producing neurons.
- Type-1 Narcolepsy
- Treatment - usually there is no cure but there are symptomatic treatments.
- Pharmacotherapy
- Modafinil is the first-line treatment for the management of hypersomnia. It is a stimulant that helps the patient to be awake.
- It is an Alpha1 agonist which helps in improving hypersomnia.
- For cataplexy, antidepressants can be used that increase the norepinephrine or serotonin tone (suppress the REM sleep).
- A regimen of forced naps at regular intervals
- The person is asked to take regular naps during the daytime so that those urges for sleep decrease and the patient may not sleep at a certain part of the day.
- Pharmacotherapy
- Klein-Levin Syndrome
- It is a rare disorder seen more in males and usually seen in early adolescence.
- Symptoms
- Hypersomnia – excessive sleepiness.
- Hyperphagia – the patient may eat a lot.
- Hypersexuality – increase in sexual activities.
- Disinhibition – behaviours like aggression may be seen.
- Symptoms
In between the episodes, the patient may be asymptomatic.
Parasomnias
- Parasomnias are disorders of partial arousal.
- These are physiological or behavioural phenomenon that occurs during or is potentiated by sleep.
- In Parasomnias, there is an overlap or intrusion of one state into the other. One state tries to intrude into the other state.
- Parasomnias can be:
- NREM-related Parasomnias
- REM-related Parasomnias
Also Read: Absence Seizures: Causes, Symptoms, Risk Factors, Diagnosis, Treatment and Complications
NREM-Related Parasomnias
- Somnambulism/Sleepwalking
- Usually occurs in the N3 stage (slow wave sleep).
- The person may engage in some motor behaviour while the person is unconscious. E.g., the person may start moving or may be involved in some complex behaviour like opening the door and going downstairs.
- These patients are difficult to awaken.
- They may appear confused if awaken and react violently.
- These are common in children and usually disappear after adolescence.
- Many times, in these disorders, a specifier may also be added which is a sleep-related eating disorder.
- They are unconscious while doing these activities.
- Treatment
- Reassurance – as seen in many of the cases it disappears spontaneously.
- Benzodiazepines may be used – they may decrease the NREM stage.
- Sleep terrors/Night terrors
- There is a sudden arousal with fearfulness. The person may scream or cry or there may be panic symptoms.
- They may appear confused when awakened.
- They are unable to recall any dream.
- Usually occurs in the N3 stage (slow wave sleep).
- Bruxism/Teeth grinding
- The person grinds the teeth and makes a loud sound which may damage the enamel
- Treatment
- The patient is asked to wear some oral appliances such as a mouth guard to protect the teeth.
- Somniloquy/Sleep talking
- The person talks during sleep and is unable to recall in the morning.
- Sleep Enuresis/Bed wetting
- The person urinates during sleep while in bed.
- There are 2 forms:
- Primary – when there is a continuance of bed wetting since infancy.
- Secondary – when there is a relapse after toilet training was completed with a period when the child remained dry.
- Usually, bed wetting resolves before 6 years of age.
- Treatment
- Behavioural techniques can be used such as Bell and Pad/Bell alarms are the treatment of choice.
- Pharmacotherapy
- Desmopressin is the drug of choice – also available as intranasal.
- Other drugs like Imipramine and Oxybutynin are also used for the management.
- The person urinates during sleep while in bed.
REM-Related Parasomnias
- Nightmare Disorder
- There is a sudden arousal and fearfulness.
- The person can recall any dream.
- Treatment
- Behavioural techniques may be used.
- Benzodiazepines may also be helpful.
- REM-Sleep Behavioural Disorders
- This is the failure of the patient to have atonia (paralysis in sleep) leading to the enacting of dreams like punching and kicking.
- The person seems unaware of the environment. They may even fall.
- Treatment
- Clonazepam is one of the Benzodiazepines that are used in management.
Assessment
- Some important techniques which are used in the assessment of sleep disorders are:
Polysomnography
- It is the recording of the physiological activity during sleep.
- This takes 6-8 hours for 1 test.
- EEG, EOG, EMG, and ECG are recorded.
- Nasal, oral flow, and nasal pressure are recorded.
- The respiratory effort (thoracic and abdominal) is also measured.
- Pulse oximeter and heart rate are monitored.
- Any activities in the leg or arms are also monitored.
- Body positions are noticed.
- Snoring is observed.
Actigraphy
- Measures and records movements.
- It is worn on a wrist like a wristwatch.
- It is used to measure sleep-wake cycles.
Sleep-wake disorders in ICD-11 have been removed from Mental, behavioural, or neurological developmental disorders and placed in a separate chapter.
Clinical Questions
Q. Which waves are seen in the transition from wakefulness to sleep?
Ans. Theta waves
Q. PGO is seen in which stage?
Ans. REM stage.
Q. What is Paradoxical sleep?
Ans. Even though the person is sleeping the EEG is showing activity similar to the awake state.
Q. What is Tonic Atonia?
Ans. It is the state which shows as if the muscle is in paralysis.
Q. What is the N3 stage of NREM called?
Ans. Deep sleep stage.
Q. What are the two types of sleep-wake disorders?
Ans. Dyssomias and Parasomnias.
Q. What are the types of Dyssomnias?
Ans. Insomnia and Hypersomnia.
Q. What are the disorders associated with Insomnia?
Ans. Restless leg syndrome, Periodic limb movement disorder.
Q. What are the disorders associated with Hypersomnia?
Ans. Narcolepsy and Klein-Levin syndrome.
Q. What are the NREM-related Parasomnias?
Ans. Somnambulism, Sleep terrors, Bruxism, Somniloquy, and Sleep Enuresis.
Q. What is Actigraphy?
Ans. It is a technique used to measure and record movements.
And that is it! That is everything you need to know about sleep disorders and its types for your Psychiatry preparation.
Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Smarter Video Lectures, Game Changing Qbank, Audio QBank, Structured Notes, Treasures, and Mock Tests for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
EEG (Electroencephalogram)
Frequency
Important Waves seen in EEG in Humans
Delta Waves (λ)
Theta Waves (θ)
Alpha Waves (α)
Beta Waves (β)
Sleep Stages
Distribution of Sleep in Young Adulthood
Various Stages of Sleep and Important Changes in EEG, EOG, AND EMG
NREM
REM: Rapid Eye Movement (Paradoxical sleep)
Differences Between NREM and REM
NREM
REM
Sleep-Wake Disorders Dyssomnia
Insomnia
Some Disorders Associated with Insomnia
Hypersomnia
Disorders Associated with Hypersomnia
Parasomnias
NREM-Related Parasomnias
REM-Related Parasomnias
Assessment
Polysomnography
Actigraphy
Clinical Questions
Q. Which waves are seen in the transition from wakefulness to sleep?
Q. PGO is seen in which stage?
Q. What is Paradoxical sleep?
Q. What is Tonic Atonia?
Q. What is the N3 stage of NREM called?
Q. What are the two types of sleep-wake disorders?
Q. What are the types of Dyssomnias?
Q. What are the disorders associated with Insomnia?
Q. What are the disorders associated with Hypersomnia?
Q. What are the NREM-related Parasomnias?
Q. What is Actigraphy?