Congenital Anomalies Of Thyroid
Feb 15, 2023

Congenital anomalies of the thyroid gland are a relatively common problem affecting approximately 1-3% of the general population. These anomalies can lead to a range of thyroid disorders, including hypothyroidism, hyperthyroidism, and goiters, and may require surgical intervention.
Surgical management of congenital anomalies of the thyroid gland can be complex and requires a good understanding of anatomy, surgical techniques, and postoperative care.
From the perspective of the NEET PG exam, congenital anomalies of the thyroid gland are an important topic that is commonly tested in the exams. Having a good understanding of this topic is essential in order to perform well.
In this blog, we have discussed congenital anomalies of thyroid in brief for NEET PG exam preparations. Read on.


What Is Thyroglossal Cyst?
A neck lump called a thyroglossal duct cyst can develop after the thyroid gland forms during fetal development. Typically, it is discovered in preschoolers or in the middle of adolescents.
Clinical Features of Thyroglossal Cyst
- Midline swelling in the anterior part of neck. Which moves with deglutition and moves up on protrusion of tongue
Diagnosis Of Thyroglossal Cyst
There are a variety of possible diagnostic procedures for thyroglossal duct cysts, including:
- Ultrasonography examination
- Blood test
- Thyroid imaging
- X-rays taken with a tiny needle and a contrast agent
Complications
- Infection of thyroglossal cyst leads to abscess formation; managed with Incision and drainage. Thyroglossal Fistula occurs as a complication of I/D. Therefore, it is an acquired condition. Thyroglossal cyst is congenital conditions. Thyroglossal cyst increases the risk for papillary Carcinoma Thyroid.
Treatment of Thyroglossal Cyst
- Treatment of choice: Sistrunk Operation (En Bloc removal of central part or body of Hyoid bone with cyst)
Endemic Goiter
- 5% people in population have goiter
Retrosternal Goiter
It is also known as Substernal / Mediastinal goiter. More than 50% of Thyroid Tissue is located below the opening of thoracic cage. Mostly asymptomatic and diagnosed incidentally on radiological investigation
Clinical features
- Dyspnea
- Dysphasia
- Hoarseness of voice
- Dilated veins over Anterior Chest wall
- Pemberton Sign is positive
Treatment of Retrosternal Goiter
- Thyroidectomy by cervical incision
Commonly used radioisotopes in thyroid disorders:
- l123 (Iodine 123)- its Half-life is 13 hours . it is Used for Diagnostic purpose only in RAI (Radioactive Iodine) Scan
- l131- its Half-life is 8 days.It is Used for Diagnostic and Therapeutic purpose in RAI scan and Ablation
- l131- it Emits β Rays (90%) and Y - Rays (10%)
|
Emits β Rays (90%) |
Emits Y - Rays (10%) |
|
|
Absolute Contraindications for Radioactive Iodine Ablation
- Pregnancy
- Lactation
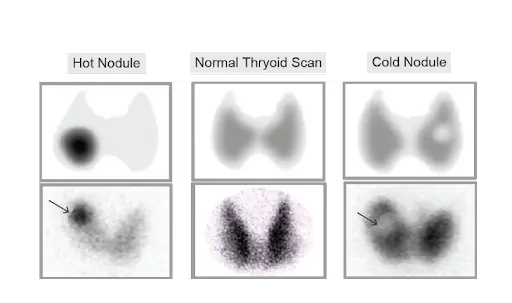
Radioactive iodine Scan aka Thyroid Scan
- Hot nodule: Increased uptake as compared to surrounding tissue- Risk of malignancy 1-3%
- Cold Nodule: Decreased uptake as compared to surrounding tissue- Risk of malignancy 17-20%

- In Graves’ Disease: In whole thyroid there is relatively increased RAI uptake
- In Toxic MultiNodular Goiter: Certain nodules having increased uptake and certain nodules having decreased uptake i.e. both hot and cold nodules are present
- In Thyroiditis: There is inflammation of thyroid. Therefore, decreased uptake of RAI i.e. <5% uptake of RAI





Types of thyroidectomy
- Total thyroidectomy: Removal of all visible thyroid tissue
- Hemithyroidectomy: Removal of one lobe with isthmus
- Subtotal Thyroidectomy: Only 3-4 gm of thyroid tissue left in each lobe superiorly
- Hartley Dunhill procedure: Modification of Subtotal Thyroidectomy 4-6 gm of tissue left in Single Lobe
- Near Total thyroidectomy: Total less than 1 gm of tissue is left near/ adjacent to Recurrent Laryngeal Nerve at Ligament of Berry
Indications
- HemiThyroidectomy: Performed in Benign disorder involving one lobe
- Total Thyroidectomy: Performed in Thyroid Malignancy and benign disorders involving both lobes
- Subtotal Thyroidectomy: Performed in Multinodular Goiter in Elderly
Solitary Thyroid Nodule
It Most common STN: Colloid Goiter > Follicular Adenoma. 1st Investigation done in STN: TFT (TSH, T3, T4) investigation of choice for Solitary thyroid nodule is FNAC.
Limitations of FNAC in Solitary Thyroid Nodule
- Follicular neoplasms: It cannot differentiate Follicular Adenoma from follicular Carcinoma. (Capsular/Follicular invasion not seen on FNAC). Riedel’s Thyroiditis: Whole thyroid is replaced by fibrous tissue
- Thyroid Lymphoma: Any lymphoma Investigation of choice is biopsy. In All of the above limitations of FNAC: Investigation of choice is Biopsy

- Most common Cause of Hypothyroidism worldwide: Hashimoto's Thyroiditis. Most common Cause of Hyperthyroidism worldwide: Grave's Disease

Grave's Disease
- Aka Diffuse Toxic Goiter.Associated with HLA-B8/DR-3. It is an Autoimmune disorder (autoimmune disorder are most commonly seen in females)
- Autoantibody: LATS (long acting thyroid stimulator). LATS antibody against TSH Receptor
- Due to increased Ab, there would be↑↑ T3 and↑↑ T4 and negative feedback causes ↓ TSH
Increased T3&T4 results in Following Clinical Features
- Thyrotoxicosis
- Ophthalmopathy
- Dermopathy: Pretibial myxedema because of deposition of glycosaminoglycan
- Acropathy: Subperiosteal new bone formation
- Gynecomastia


Clinical Features of Graves Disease
|
Sympathetic Stimulation S/S |
Thyroid Stimulation S/S |
Female Specific S/S
Children Specific S/S
In young patients
In Elderly
|
|
In Thyroid gland
- Thyroid Hyperactive: ↑↑ Radioactive Iodine Uptake
- Thyroid Hyper vascular: Most prominent at upper pole-palpable thrill, audible Bruit, venous Hum
Diagnosis
- Eye Signs present in patients of Hyperthyroidism are Diagnostic
- Single Investigation that confirms diagnosis: Presence of autoantibodies
Management
- For Sympathetic S/S 1st drug given: Propranolol
- Antithyroid drugs: To control over production of T3 &T4
Antithyroid Drugs
- Methimazole: Diagnosis of choice in Graves (S/E: ↑↑ risk of Choanal Atresia, Agranulocytosis and Aplasia Cutis. Therefore, not safe in pregnancy)
- Carbimazole: Diagnosis of choice in pregnancy
- Propylthiouracil: Diagnosis of choice in Thyrotoxic crisis as it Blocks Peripheral Conversion (S/E: ↑↑ risk of Hepatic failure especially in females and children)
- The drugs are given to patient to make the patient euthyroid before surgery
- Treatment of choice in Grave's: Total Thyroidectomy
- RAI Ablation
Also Read: Hyperthyroidism Symptoms
To study this topic in detail, download the PrepLadder app and get access to engaging video lectures and study notes for preparation.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
What Is Thyroglossal Cyst?
Clinical Features of Thyroglossal Cyst
Diagnosis Of Thyroglossal Cyst
Complications
Treatment of Thyroglossal Cyst
Endemic Goiter
Retrosternal Goiter
Clinical features
Treatment of Retrosternal Goiter
Absolute Contraindications for Radioactive Iodine Ablation
Radioactive iodine Scan aka Thyroid Scan
Types of thyroidectomy
Indications
Solitary Thyroid Nodule
Limitations of FNAC in Solitary Thyroid Nodule
Grave's Disease
Increased T3&T4 results in Following Clinical Features
Clinical Features of Graves Disease
In Thyroid gland
Diagnosis
Management
Antithyroid Drugs
Top searching words
The most popular search terms used by aspirants
- NEET PG Surgery