Pancreatic Cancer: Neuroendocrine Tumors of Pancreas
Jun 29, 2023

The pancreas is an organ in the abdomen, situated behind the lower part of the stomach. The pancreas tissues are where pancreatic cancer first manifests itself. Along with producing digestive enzymes, the pancreas also produces hormones that aid in blood sugar regulation.
In addition to other growths, the pancreas may develop tumors that are cancerous or benign. The most common type of pancreatic cancer, pancreatic ductal adenocarcinoma, arises in the cells lining the ducts that drain the pancreas digesting enzymes.
In its initial stages, when it is most curable, pancreatic cancer is rarely discovered. This is because symptoms frequently don't manifest themselves until the disease has spread to other organs.
The Most common genetic mutation in the Carcinoma pancreas is K-RAS > p–16.
Read this blog further to get a quick overview of this important topic Pancreatic Cancer: Risk Factors, Clinical Features, Diagnosis, Treatment, Neuroendocrine Tumors of Pancreas for SURGERY to ace your NEET PG exam preparation.

Risk Factors of Pancreatic Cancer
Below are mentioned few of the risk factors for pancreatic cancer:
- Smoking or tobacco
- Hereditary Factors or genetic susceptibility [H3-AFP]
- Hereditary pancreatitis
- HNPCC (hereditary non-polyposis colon cancer)
- Hereditary Breast and Ovarian Cancer (associated with BRCA - 2)
- Ataxia Telangiectasia
- Familial atypical multiple mole melanoma (FAMMM) syndrome
- Peutz-Jeghers Syndrome
Causes of Pancreatic Cancer
The exact cause of pancreatic cancer is unknown. Smoking and having specific inherited gene mutations are two factors that have been linked to an increased risk of this type of cancer.
Symptoms of Pancreatic Cancer
Pancreatic cancer signs and symptoms frequently don't appear until the disease has progressed. They may consist of:
- Back discomfort that originates in the abdomen
- Appetite loss or unintentional weight loss
- Jaundice
- Pale colored stools
- Dark Urine
- Skin itching
- Newly discovered diabetes or diabetes that is already present but becomes harder to control
- Clots of blood
- Fatigue
- Most common symptom is Jaundice > weight loss.
- The most common symptom of Carcinoma head of the pancreas is Jaundice > weight loss.
- The most common symptom of Carcinoma Body and Tail Pancreas is Weight loss.
- Ampullary Carcinoma- Its most common symptom is Jaundice. Waxing and waning of jaundice with melena (seen every 2-3 months in 1/3rd cases)
| Important Information TROUSSEAU Syndrome - Migratory Superficial Thrombophlebitis seen in Malignancy (most commonly associated with carcinoma pancreas) TROUSSEAU Sign - Carpopedal Spasm in Hypocalcemia TROISIER’S Sign - Left Supraclavicular Lymphadenopathy (Virchow’s Node or signal node) |
Diagnosis
- Investigation of choice for Carcinoma pancreas is CECT
Radiological Signs
- Carcinoma head of the pancreas on Barium study
- 1. Antral pad signs

2. Widening of C loop
3. Reverse 3 Sign of Frost Berg

4. Double Duct Sign

- Other signs in Carcinoma pancreas
- Rose-thorn Appearance
- Mucosal Irregularity
- Scrambled Egg Appearance
Treatment of Pancreatic Cancer
- For Carcinoma Body and Tail Pancreas – Distal pancreatectomy is done.
- For Benign tumor in the head of Pancreas – Enucleation is done
- Carcinoma head of Pancreas
- Whipple’s procedure - Pancreaticoduodenectomy (PD)
- Longmire traverso procedure - Pylorus preserving Whipple’s procedure
- For advanced or metastatic stage Gemcitabine is given

| Whipple’s procedure | Long wire traverso procedure (pylorus preserved) |
| 1st anastomosis is Pancreaticojejunostomy 2nd anastomosis is Hepaticojejunostomy 3rd anastomosis is Gastrojejunostomy | 1st anastomosis is Pancreaticojejunostomy 2nd anastomosis is Hepaticojejunostomy 3rd anastomosis is Duodenojejunostomy |
Performed in anticlockwise fashion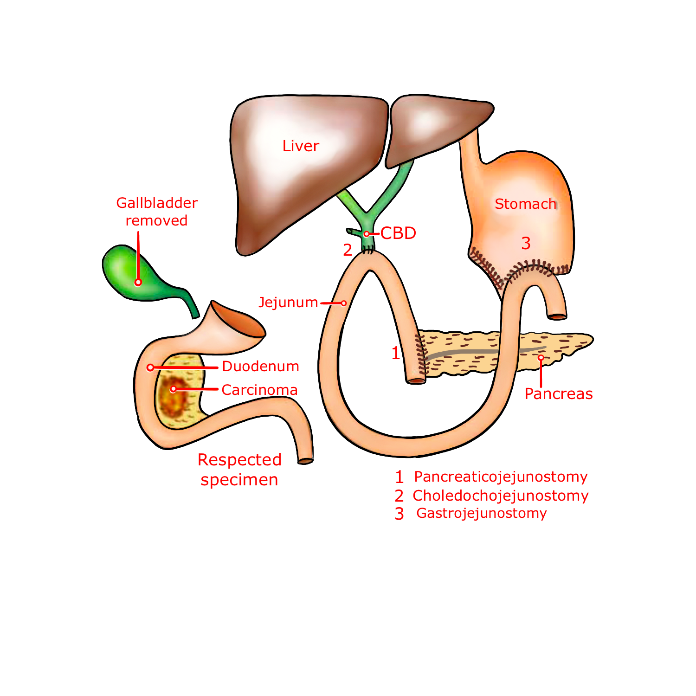 |  |

The most common site of anastomotic leak is Pancreaticojejunostomy (PJ) > Gastrojejunostomy (GJ) > Hepaticojejunostomy (HJ).
Most common complication of Pancreaticoduodenectomy is Delayed gastric emptying.
Most common cause of death after Pancreaticoduodenectomy is Cardio-pulmonary complications.
Most important predictor of survival is R0 resection. Types of resections
- R0 resection – negative margin
- R1 resection – microscopic positive margin
- R2 resection – macroscopic positive margin
Most important margin in Pancreaticoduodenectomy is the Uncinate margin or Retroperitoneal margin or Superior mesenteric vessel margin. Survival in Carcinoma Pancreas
- Stage I and II is 16-20 months
- Stage III is 6-10 months
- Stage IV is 3-6 months
Neuroendocrine Tumors (Net) of Pancreas
A category of malignancies known as pancreatic neuroendocrine tumors (pNET) can develop in the pancreas hormone-producing cells. Islet cell malignancies, commonly known as pancreatic neuroendocrine tumors, are extremely uncommon.
Small hormone-producing cells (islet cells), which are often present in your pancreas, are where pancreatic neuroendocrine tumors start.
Some pancreatic neuroendocrine tumor cells continue to secrete hormones, these tumors are referred to be functional tumors because they cause the body to produce an excessive amount of a particular hormone. Gastrinoma and glucagonoma are a couple of examples of these types of tumors.
These tumors are sometimes referred to as nonfunctional tumors since they rarely secrete an excessive amount of these hormones.
- Most common Neuroendocrine tumor of Pancreases is Non-Functional pancreatic polypeptide cell tumor (PPOMA)
- Most common functional Neuroendocrine tumor of the Pancreas is Insulinoma
- Most common functional and Malignant Neuroendocrine tumors of the Pancreas is Gastrinoma
- Neuroendocrine Tumors are symptomatic because of production of active substances. So, patients are
- Symptomatic at an early stage
- Diagnosed at an early stage
- Treated at an early stage
- Better prognosis - Neuroendocrine tumors > Adenocarcinoma
Diagnosis
- Diagnosed is made in Laboratory by measuring active substance or its by-product
- Investigation of choice for localization of Neuroendocrine tumors: SRS (Somatostatin receptor Scintigraphy) (as all Neuroendocrine tumors express Somatostatin receptors except Insulinoma)
- Most common site of metastasis is Liver

Insulinoma
Insulinoma is one of several pancreatic neuroendocrine tumors (pNET) or islet cell tumors. These are uncommon cancers that originate in your pancreas' endocrine cells. They affect the endocrine cell that makes the hormone insulin, which controls the rise of your blood sugar (blood glucose) levels. More than 90% of insulinomas are benign tumors since they don't spread outside of your pancreas. Surgery is performed by medical specialists to treat and remove insulinomas.
It is the most common functional Neuroendocrine tumor of the Pancreas and is mostly Benign. The Most common site is equally distributed in the Head, Body, and Tail. In 5% of cases, it is associated with MEN-1. In MEN-1 insulinoma is malignant and has multiple lesions.
Clinical Features of Insulinoma
- Characterized by Whipple’s Triad
- Symptoms of Hypoglycemia
- Blood glucose (45 – 50 mg/dl)
- Improvement in symptoms after taking oral glucose
- Neuroglycopenic symptoms
- Sympathetic overactivity leading to
- Tachycardia
- Palpitation
- Excessive sweating
- Tremors
- It is a Painless condition associated with weight gain.
Diagnosis of Insulinoma
Gold Standard Investigation is 72 hours fasting. Insulin/ Glucose (ratio) more than 0.4 is diagnostic. The best pre-operative Test for localization is Intra Arterial Calcium injection with portal venous blood sampling. Overall best Investigation for localization is EUS (endoscopic ultrasound ) along with “Intra–Operative Palpation”.
Treatment of Insulinoma
- For preoperative preparation, Diazoxide is given as it is directly toxic to beta-pancreatic cells so it decreases the insulin
- For the Body and Tail Tumor - Distal Pancreatectomy is done
- For head Tumor– Enucleation (since it’s benign) is done

Gastrinoma or Zollinger Ellison Syndrome
Gastrinomas are neuroendocrine tumors (NETs) that secrete gastrin and lead to the clinical illness known as Zollinger-Ellison syndrome (ZES). They are typically found in the duodenum or pancreas. Nearly equally frequently, a lot of gastrinomas form in the pancreas or the duodenum, and around 10% form as primary neoplasms in the lymph nodes of the pancreaticoduodenal region (gastrinoma triangle).
The majority of gastrinomas (75–80%) are sporadic, but 20–25% of them are connected to MEN-1, or multiple endocrine neoplasia type 1. More than 50% of gastrinomas are cancerous, and they can spread to the liver and local lymph nodes. Multiple endocrine neoplasia type 1, Zollinger-Ellison syndrome, and peptic ulcer disease are linked to one-fourth of gastrinomas.
It is the most common functional and Malignant Neuroendocrine tumor of the Pancreas. The most common site is Duodenum > Pancreas.
In Duodenum Most common site is 1st part > 2nd part > 3rd part (4th part is not Involved). 75% sporadic and 25% associated with MEN 1. In all of the cases of Gastrinoma in MEN-1 common site is duodenum
90% of gastrinoma is present in the Triangle of Passaro’s or Gastrinoma triangle. Boundaries of Passaro’s Triangle are:
- Junction of Cystic duct and CBD
- Junction of Second and the third part of duodenum
- Junction of neck and body of pancreas
It has increased Gastrin production leads to increase production of Acid causing Peptic Ulcer Disease:

Clinical Features of Gastrinoma
- Most common symptom is Abdominal pain
- Other symptoms include
- Retrosternal heartburn
- Dyspepsia
- Diarrhea (acid induced): Nasogastric aspiration halts Acid induced Diarrhea
- Has large ulcers or multiple ulcers or Jejunal ulcers or Refractory ulcers
Diagnosis of Gastrinoma
- Gastrin more than 1000 Pg/ml is diagnostic
- Basal Acid Output (BAO) more than 15 mEq/hour is also diagnostic
- Best Provocative Test is Secretin Stimulation Test (release of gastrin more than 200 Pg/ml)
- Investigation of choice for localization is Somatostatin receptor scintigraphy (SRS)
Treatment of Gastrinoma
- Drug of choice is Proton pump inhibitors
- Treatment of choice is Pylorus preserving Whipple’s procedure
Surgery Related Articles:
Glucagonoma or Hyperglycemic Cutaneous Syndrome
Pancreatic glucagonoma is an uncommon type of tumor. The pancreas releases glucagon, a hormone that collaborates with insulin to regulate blood sugar levels.
Large amounts of glucagon are produced by glucagonoma tumor cells, and these high levels cause severe and perhaps fatal symptoms.

- It is Also known as “4” D Syndrome
- Diabetes Mellitus
- Dermatitis - Necrolytic Erythema Migrans (Most common symptom)
- Deep vein thrombosis
- Depression
- Most common site of Tumor is Body and Tail of Pancreas
Diagnosis of Glucagonoma
- Investigation of choice is increased Glucagon levels
- Investigation of choice for localization is SRS (Somatostatin Receptor Scintigraphy)
Treatment- of Glucogonoma
As in glucagonoma the Tumor is located in body and tail, so we do Distal Pancreatectomy
Vipoma (Vasoactive Intestinal Peptide Tumor)
It is also known as Verner Morrison Syndrome or Pancreatic Cholera or WDHA Syndrome. There is an increase in VIP (Vasoactive Intestinal Peptides) which will lead to an increase in secretions causing watery diarrhea.
WDHA Syndrome includes:
- Watery Diarrhea (4 – 6 Liters) leading to Loss of sodium, chloride, potassium, and bicarbonate Increased Random blood sugar, and calcium (Hyperglycemia and Hypercalcemia)
- Hyperkalemia
- Achlorhydria
The Most common site of occurrence is Tail and It is a medical emergency
Diagnosis of Vipoma
- Diagnosis is based on VIP (Vasoactive Intestinal Peptides) levels
- Investigation of choice for localization is SRS (Somatostatin Receptor Scintigraphy)
Treatment of Vipoma
- Treatment of choice is Distal Pancreatectomy
Cystic Neoplasm of Pancreas
Most common Cystic lesion of Pancreas is Pseudocyst (75%). The most common Cystic Neoplasm of the Pancreas is Mucinous Cystadenoma (MCN).
Serous Cyst Neoplasm or Adenoma (SCN):
Generally, it is Benign. The most common site of occurrence of serous cystic neoplasm is in the Head of the Pancreas. It is most commonly seen in females (5th-6th decade)
Pathological features of serous cystic neoplasm
Individual cyst in SCN (Serous Cyst Neoplasm) is Microcystic and has a Sponge-like or honeycomb appearance
Clinical Features of serous cystic neoplasm
Majority of the patients are asymptomatic. In symptomatic patients have Vague abdominal pain
Diagnosis of Serous Cystic Neoplasm of Pancreas
- Investigation of choice is CECT
- On CECT
- Central Stellate scar
- Central Sunburst Calcification

Treatment of serous Cystic Neoplasm Of Pancreas
- Observation
- Resection is indicated if
- Diagnostic uncertainty
- Symptomatic
- Size is more than 4 cm
- On aspiration of Cyst content
- Content is Serous
- CEA is decreased
- Amylase is decreased
Mucinous Cyst Neoplasm or Adenoma

It is the most common cystic Neoplasm of the pancreas. It is a premalignant condition. It is mostly common in females (5th-6th decade). The most common site is the Body and Tail of the Pancreas. It is Macrocytic. Most patients are symptomatic and have Vague abdominal pain.
Diagnosis of Mucinous Cyst Neoplasm
- Investigation of choice is CECT (shows Peripheral Egg Shell Calcification)
Treatment of Mucinous Cyst Neoplasm
- Surgical Resection of Tumor in all the cases
- On aspiration of Cyst content
- Content is mucin
- CEA is increased
- Amylase is decreased
IPMN – Intraductal Papillary Mucinous Neoplasm
It is a premalignant condition. It is common in both males and Females (6th and 7th decade). The most common site is the Head and Uncinate process. There is excessive secretion of mucin, and the whole pancreatic duct gets distended with the mucin causing obstruction.
It has 3 Types:
- Main duct variety
- Side branch variety
- Mixed variety
Clinical features of IPMN
- Recurrent attack of acute pancreatitis
Diagnosis of IPMN
- Investigation of choice is Endoscopy
- On Endoscopy - Mucin extruding from Fish-Mouth Opening

Treatment of IPMN
- Partial pancreatectomy
- On aspiration of Cyst content
- Content is mucinous
- CEA is increased
- Amylase is increased

Download the PrepLadder App and get the best neet pg online coaching with world-class video lectures, QBank, Mock Tests and more!
Download PrepLadder's best app for neet pg preparation for Android
Download PrepLadder's best app for neet pg preparation for ios

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Risk Factors of Pancreatic Cancer
Causes of Pancreatic Cancer
Symptoms of Pancreatic Cancer
Diagnosis
Radiological Signs
Treatment of Pancreatic Cancer
Neuroendocrine Tumors (Net) of Pancreas
Diagnosis
Insulinoma
Clinical Features of Insulinoma
Diagnosis of Insulinoma
Treatment of Insulinoma
Gastrinoma or Zollinger Ellison Syndrome
Clinical Features of Gastrinoma
Diagnosis of Gastrinoma
Treatment of Gastrinoma
Glucagonoma or Hyperglycemic Cutaneous Syndrome
Diagnosis of Glucagonoma
Treatment- of Glucogonoma
Vipoma (Vasoactive Intestinal Peptide Tumor)
Diagnosis of Vipoma
Treatment of Vipoma
Cystic Neoplasm of Pancreas
Serous Cyst Neoplasm or Adenoma (SCN):
Mucinous Cyst Neoplasm or Adenoma
IPMN – Intraductal Papillary Mucinous Neoplasm
Treatment of IPMN
Top searching words
The most popular search terms used by aspirants
- NEET PG Surgery