Nasal Polyps : Causes, Symptoms and Treatment : NEET PG ENT
Feb 25, 2025

Nasal polyps are soft, painless, noncancerous growths on the lining of the nasal passages or sinuses. Are they dangerous? That is debatable but they are definitely a huge inconvenience because they can interfere with the normal ventilation and drainage of the sinuses.
Nasal Polyps is an important topic for your ENT preparation.
Definition: A polyp is chronically inflamed oedematous tissues. Whenever the tissues are chronically inflamed and become oedematous, the tissue prolapses into a hollow cavity, which is the nasal cavity, which is a nasal polyp. The polyp will be named according to the site where there is inflammation, making the tissue become oedematous and prolapse into a hollow cavity.
- Benign: Polyps are benign lesions of the nasal cavity and are not malignant.
- Types: In the paranasal sinuses, the two types of polyps are:
- Antrochoanal Polyp- The disease is starting from the maxillary area and goes into the choana posteriorly.
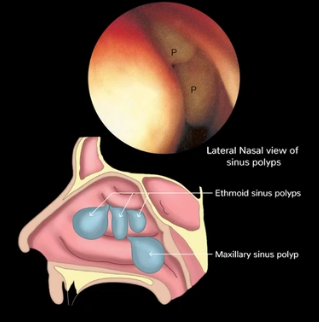
- Ethmoidal Polyp- These are coming from the ethmoidal air cells.

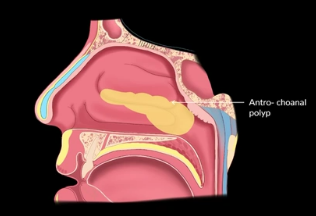
Antrochoanal Polyp
Origin
- The "antro", comes from antra; and the "choanal" from choana. These polyps originate in the maxillary antrum, go into the nasal cavity, and are directed posteriorly toward the choana.
Extent
- The extent of this polyp is posteriorly towards the choana and not anteriorly towards the nasal vestibule.
The three parts of the polyp are
- The Antral part: This is in the maxillary antrum from where it originates.
- The Nasal part: It goes into the nasal cavity.
- The Choanal part: From the nose, it goes into the choana (communication between the nose and the nasopharynx) posteriorly.
- Single/Unilateral: Antrochoanal polyps are single polyps. This is a one-unit polyp present in one side of the nasal cavity or sinuses. It is not bilateral.
- Age: It is often seen and younger individuals.
- Male Predominance
- Cause/Etiology: The cause for these kinds of polyps is infection and not an allergy.
The organism responsible for causing this polyp is streptococcus pneumonia.
Also read: Anatomy of Middle Ear - NEET PG ENT
Clinical Features/Symptoms
- When there is a unilateral mass in the nasal cavity, the symptoms experienced by the patient are:
- Nasal obstruction: There will be a nasal obstruction and difficulty in breathing because there is a mass that is occluding the nasal cavity.
- Nasal discharge: There is edema and inflammation which has resulted in the polyp. The normal major secretions are not able to drain posteriorly because the mass is occluding it.
- Hyposmia/Anosmia: The air that is reaching the cribriform plate will get reduced because there is some mass that is occluding the nasal cavity.
- Rhinolalia Clausa: The nose acts as a resonator that ensures a good quality of voice. When the nasal block will be causing hypotonic voice(Nasal Twang). Rhinolalia Clausa will happen because the nasopharynx is closed, and there will be nasal intonation in the voice.
- Hampered Ventilation: When the air is going into the choana or posteriorly into the nasopharynx, ventilation that reaches the nasopharynx will be hampered. Ventilation via the Eustachian tubes to the middle ear will also be hampered and will result in middle ear diseases like nonsuppurative otitis media. This is not an infective condition but is rather noninfective. The disease will be unilateral because the polyp is unilateral.
Also read: Disorders of Nose and Paranasal Sinus - NEET PG ENT
On Examination
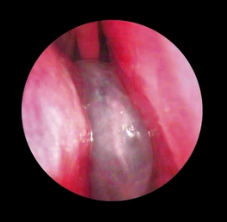
On anterior rhinoscopy: A greyish-white mass can be seen in the nasal cavity. Typically, this cannot be seen going into the choana but can be seen with the help of posterior rhinoscopy (A mirror has to be used behind the uvula. In the mirror one has to look at the reflection of the polyps that are present in the choana or nasopharynx, that can be seen in the mirror.) The posterior rhinoscopy is done to assess the spread posteriorly .
- Whenever there is a unilateral nasal mass, a differential diagnosis may be carried out. As per the age, the differential diagnosis may vary.
- If the diagnosis is of a child or a young individual, one must think of congenital lesions, typically meningocele or meningoencephalocele (Their appearance resembles that of a polyp). Others may consist of a glioma or a dermoid.
- If the symptoms are seen in a juvenile/adolescent age group, one must rule out a juvenile nasopharyngeal angiofibroma. This can also present as a unilateral mass in the nasal cavity, with nasal obstruction, difficulty in breathing, hypotonic voice, hyposmia, and unilateral middle ear disease. On examination, it is not greyish white but a red and vascular mass. The difference between JNA and an AC polyp is AC polyp never presents with bleeding from the nose (spontaneous, recurrent, unprovoked, provoked, profuse epistaxis- these are not features of AC polyp that are definite features of JNA.)
- If the same thing is seen in older individuals, any other type of malignancy or benign tumors such as inverted papilloma.
- Imaging: Initially, an x-ray can be done but it cannot provide specificity to understand the extent of the disease. It only has a good sensitivity to pick up the disease. A Non-Contrast CT Scan of the nose and para nasal sinuses is thus the best option initially for a patient with nasal polyp. This scan can help understand the extent and origin of the polyp, if there are any bony erosions around it, and if there is a disease extending beyond the choana or nasopharynx. After the scan further investigation can be carried out to rule out other differential diagnoses.
Treatment
- No role of medical therapy: There is no role in medical therapy for patients with AC polyps. Antibiotics can be given to clear the infection, but the inflamed edema that has prolapsed into the nasal cavity, going to the choana will not disappear with antibiotics.
- Surgery has to be performed: The surgery of choice is Functional Endoscopic Sinus Surgery. It is called functional because only diseased tissues are removed and not the normal tissue. Removal is done with the help of an endoscope. The medical procedure takes place by going into the sinus. As much normal mucosa as possible is preserved.
- Whenever such a surgery is performed, before proceeding, the unilateral nasal mass has to be palpated to check if it is bleeding on touch.
- One has to take a syringe and aspirate and see if they are getting any fluid. If there is bleeding on touch, there is the probability of a tumor like an inverted papilloma. If the patient is in an adolescent age group, one must think of angiofibroma. This will lead to a change of surgical plans and approach to the patient.
- If there is fluid on aspiration, it is either a meningocele or meningoencephalocele. One has to be extra careful while performing surgery otherwise it can lead to intracranial complications.
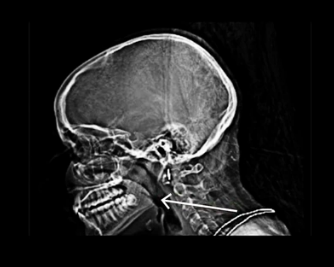
Crescent Sign
- A crescent sign is seen in a patient with an AC polyp. There is a mass coming from the maxillary sinus that is going into the nasal cavity and nasopharynx. There is a column of air present between the mass and the posterior pharyngeal wall called the crescent sign or Dodd's sign. A lateral view is supposed to be studied to find out if this sign is present. In malignancy or tumors, or JNA, this sign is absent.
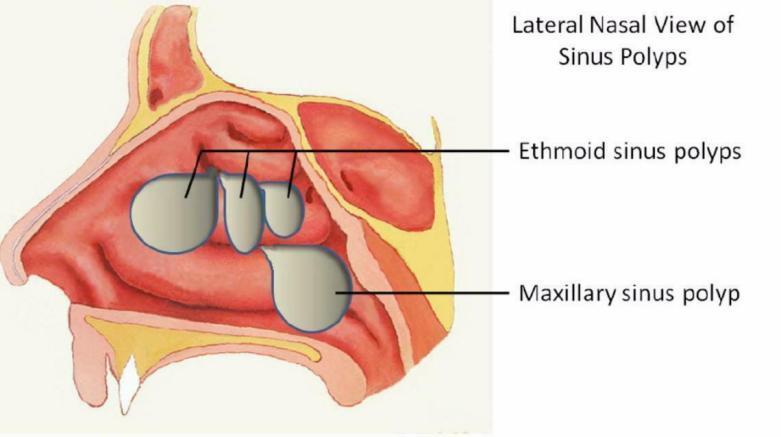
Ethmoidal Polyps
Origin
- As the name suggests these are originating from the Ethmoidal air cells. The anatomy of these air cells shows that they are sandwiched in between the frontal sinus anteriorly, and those sphenoid sinuses posteriorly. From the Ethmoidal air cells, there are inflamed tissues which are the Ethmoidal polyps. These polyps grow anteriorly.
Extent
- The extent of the spread of the disease is anterior and not posterior
- Age: This disease is typically seen in adults and middle-aged groups.
Etiology
- These polyps are caused by allergic origin or diseases of ciliary motility. In ciliary disorders, the mucociliary clearance (not just of the nose and paranasal sinuses, but up to the trachea, alveoli, bronchus, and into the lungs, causes bronchiectasis, sinusitis, etc.)
- There are certain syndromes associated with ciliary motility defects. These polyps are associated with certain syndromes:
- Chronic rhinosinusitis
- Asthma
- Cystic fibrosis
- (MCQ) Kartagener's syndrome: Bronchiectasis, sinusitis, situs inversus.
- (MCQ) Young syndrome: Sinopulmonary syndrome and azoospermia.
- (MCQ) Churg Strauss syndrome: Asthma, fever, eosinophilia, vasculitis, granuloma.
Sampter's Triad
- Asthma
- Aspirin sensitivity (to be avoided in patients with nasal polyposis as it can cause a reaction that can be fatal to the patient).
- Nasal polyposis
Diagnosis
- The symptoms will be the same as that of an AC polyp. It is the local manifestation of systemic disease. Since allergy is present in both nasal cavities, ciliary motility disorder will happen in both, so ethmoidal polyps are bilateral.
- There will be a bilateral nasal obstruction and difficulty in breathing.
- Bilateral nasal intonation in the voice
- Bilateral hyposmia
- Eustachian tube blocked (bilateral)
- Excessive sneezing
- Anosmia
- Snoring
- Headache
- Bilateral middle ear disease
Examination
- In this case, an anterior rhinoscopy is sufficient since these polyps are growing anteriorly, it is not mandatory to do a posterior rhinoscopy.
- Typically, pale oedematous tissue with multiple pedunculated masses insensitive to touch and bleeding, which are resembling a bunch of grapes, is a hallmark of the ethmoidal polyp.
Treatment
- Before treatment diagnosis is very important. X-ray and non-contrast CT scan or the diagnosis of choice. CT Scan is more sensitive and specific and is the investigation of choice.
- These polyps are recurrent because they are allergic in origin and associated with ciliary mortality disorder.
- Investigation for allergy with elevated serum IgE levels elevated eosinophil count, and absolute eosinophil count is to be looked for.
- For the diagnosis of a ciliary motility disorder, there are multiple tests. Typically, a Saccharin test is performed where a drop of saccharin is placed in the nose. If the patient is unable to have that sweet taste in the mouth after a certain time, there is a ciliary motility defect because of which it is not going into the nasopharynx. This test is done in an OPD just to assess if there is proper ciliary motility function.
- The other test carried out is Nasal Nitric Oxide measurement. Nitric oxide is usually produced by para-nasal sinuses. This nitric oxide will be elevated in patients suffering from ciliary motility disorder.
- For cystic fibrosis, a Raised Sweat chloride test is performed.
- Along with this Raised Trans-Nasal Electrical Epithelial potential difference in an electron microscopy test will tell if there is a probability of cystic fibrosis.
- Gene and DNA analysis will again confirm the presence and absence of any genetic abnormality that is associated.
- For Treatment, a patient suffering from ethmoidal polyps is given medical therapy. There is chronic inflammation, and allergic in etiology most often.
- Treatment is started with a short course of systemic steroids, topical intranasal steroids along with anti-histamines, and nasal decongestants.
- After medical therapy, there is revaluation because there is a possibility of the polyps shrinking in size or disappearing altogether.
- If they are still present there has to be an operation and surgery. The type of surgery performed here is Functional Endoscopic Sinus Surgery. Only the polyps are removed and the normal nasal tissue is preserved. Purification of air and humidification of air, which are the normal functions of these tissues, are going to be preserved. Only the diseased mucosa is removed.
- Earlier for AC polyps, a Caldwell-Luc approach was taken where the doctors went through the sub-labial incision, elevate the mucoperiosteum over the maxilla, and enter the maxillary sinus. A front-ethmoidectomy external was also performed to reach the sinuses. Today these are obsolete. Most of the patients are managed with FESS.
Causes of Polyps
Allergy
- The prevalence of allergy in patients with nasal polyps varies from 10% - 64%.
- Elevated levels of immunoglobulin E (IgE) and positive skin tests for inhalant allergens have been determined in the majority of patients with nasal polyps.
- If allergy is not treated in patients with allergies, chances of recurrence is high.
- Treatment for nasal polyp with allergies is combination therapy, single therapy usually fails.
Bacteria
- Gram-positive organisms, including streptococci, coagulase negative staphylococci, and staphylococcus aureus, can cause polyposis.
- Moraxella catarrhalis, Haemophilus influenza, Prevotella species, Enterobacter species, and Pseudomonas species can also cause polyposis.
- Polyposis happens secondary to formation of the biofilms.
- Biofilms are the bacteria that are enclosed within a self-developed matrix of polysaccharides, which renders the bacteria inaccessible to antimicrobial agents.
- Clinically, cases of nasal polyps with the presence of biofilms may be associated with a more severe form of the disease and worse postoperative outcomes.
- Treatment – Antimicrobials that can break the biofilm and cycle of chronic inflammation secondary to infection.
- If only mechanical debridement is done, chances of recurrence are high.
Associated Disease
- Nasal polyps can occur secondary to other diseases like allergic fungal rhinosinusitis.
- Allergic fungal rhinosinusitis is a type 1 hypersensitivity reaction to fungal antigens in which patients usually have unilateral (less common) or bilateral nasal polyps.
- Approximately 80% of patients with fungal sinusitis have nasal polyps.
- In 1994, Bent Kuhn published their diagnosis criteria centred on the histological, radiographic, and immunologic characteristics of the disease.
- CT findings of AFRS– Heterogenous densities/double densities.
- Patients should have 2 major criteria or 1 major criteria with 2 minor criteria for diagnosis.
Asthma
- Patients with nasal polyps are shown to have asthma, and there is a direct association between asthma severity and the presence of nasal polyps.
- The improvement in lower airway disease is observed when nasal polyps are effectively treated.
Aspirin-exacerbated Respiratory Disease (AERD, SAMTER’S TRIAD)
- The combination of bronchial asthma, nasal polyposis and aspirin sensitivity are well described in the otolaryngology literature.
- Avoid giving salicylates and aspirin in AERD patients.
- Aspirin can cause bronchoconstriction and gradually worsens both asthma and polyposis.
- It can cause recurrence and severe form of asthma.
- The nasal polyps associated with AERD/Samter’s triad are often very extensive, with significantly higher radiological CT scores than non-AERD patients with nasal polyp.
Cystic fibrosis
- Cystic fibrosis (CF) is an autosomal recessive disorder caused by mutations of a gene on chromosome 7.
- Examination of CF patients with nasal polyps usually reveals bilateral polyposis with thick rhinorrhoea and facial deformities such as hypertelorism.
- In addition to nasal polyps, CT scan findings include hypoplasia of the frontal or sphenoid sinuses as well as demineralization and medial displacement of the uncinate process.
Primary Ciliary Dyskinesia
- Primary ciliary dyskinesia (PCD) is a rare autosomal recessive disease in which abnormal or absent beating of cilia hinders normal mucociliary clearance.
- Due to hinderance in clearance, there will be a stasis of secretions which will be a source of inflammation and polyp.
- Commonest presentations are in the upper and lower respiratory tracts, with mucus retention and recurrent infection leading to nasal polyposis and/or bronchiectasis.
Young’s syndrome
- Young’s syndrome is a rare disease consisting of three components: obstructive azoospermia, bronchiectasis, and sinus disease.
EGPA (Churg Strauss)
- Previously known as Churg Strauss syndrome, this entity has now been recognized by the 2022 revised nomenclature for vasculitides as eosinophilic granulomatosis with Polyangiitis (EGPA).
- It is a systemic small vessel vasculitis associated with asthma and eosinophilia.
- It has three phases.
- The first phase is prodromic phase i.e., the allergic phase characterized by asthma and rhinosinusitis.
- The second phase is an eosinophilic phase, hallmarked by peripheral eosinophilia and organ involvement.
- The third phase is a vasculitic phase with clinical manifestations due to small vessel vasculitis.
Comparison of Antrochoanal Polyp and Ethmoidal Polyp
Antrochonal polyp Ethmoidal polyp Age Young Middle and adult Etiology Infection Allergy Number Single Multiple Laterality Unilateral Bilateral Origin Maxilary sinus Ethmoid sinus Growth Posteriorly Anteriorly Medical Treatment No role In initial phase Surgery FESS FESS Recurrence Less High 
Important Points to Remember
- Nasal polyps can cause severe symptoms and can have a significant impact on quality of life.
- Although known to be associated with chronic inflammation the exact aetiology remains elusive.
- Nasal polyps are associated with many chronic conditions including asthma, aspirin, exacerbated respiratory disease, and cystic fibrosis.
- Nasal polyps can be easily diagnosed with anterior rhinoscopy and nasendoscopy.
- Combined medical and surgical treatment is recommended for long-term control of symptoms.
- Unilateral nasal polyps should be treated as suspected malignancy until a biopsy proves otherwise.
Frequently Asked Questions
Q: What is a Crescent Sign?
Ans. A crescent sign is seen in a patient with an AC polyp. There is a mass coming from the maxillary sinus that is going into the nasal cavity and nasopharynx. There is a column of air present between the mass and the posterior pharyngeal wall called the crescent sign or Dodd's sign. A lateral view is supposed to be studied to find out if this sign is present. In malignancy or tumors, or JNA, this sign is absent.
Q: What is Sampter's Triad?
Ans. Sampter’s triad includes:
- Asthma
- Aspirin sensitivity (to be avoided in patients with nasal polyposis as it can cause a reaction that can be fatal to the patient).
- Nasal polyposis
Q: Ethmoidal polyp is associated with all the syndromes except?
- Kartagener's syndrome
- Young syndrome
- Down’s syndrome
- Churg Strauss syndrome
Ans. Down’s Syndrome
Q. Why are polyps reoccrant in nature?
Ans. The polyps are recurrent because they are allergic in origin and associated with ciliary mortality disorder.
And that is it! That is everything you need to know about nasal polyps for your ENT preparation. For more interesting and informative posts like these, keep reading PrepLadder blogs!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Antrochoanal Polyp
Origin
Extent
The three parts of the polyp are
Clinical Features/Symptoms
On Examination
Treatment
Crescent Sign
Ethmoidal Polyps
Origin
Extent
Etiology
Sampter's Triad
Diagnosis
Examination
Treatment
Causes of Polyps
Allergy
Bacteria
Associated Disease
Asthma
Aspirin-exacerbated Respiratory Disease (AERD, SAMTER’S TRIAD)
Cystic fibrosis
Primary Ciliary Dyskinesia
Young’s syndrome
EGPA (Churg Strauss)
Comparison of Antrochoanal Polyp and Ethmoidal Polyp
Important Points to Remember
Frequently Asked Questions
Top searching words
The most popular search terms used by aspirants
- NEET PG ENT Preparation
- NEET PG Strategy