Acute Respiratory Distress Syndrome- NEET PG Medicine
Apr 5, 2023

Get ready to elevate your Medicine preparation because today you are going to learn about Acute Respiratory Distress Syndrome, which is an important topic in your Medicine syllabus.
What is Acute Respiratory Distress Syndrome? It is a condition where fluid gets collected in the air sacs of the lungs and deprives the body of oxygen. In such cases, patients suffer from shortness of breath and are unable to breathe on their own.
Let’s learn more about this syndrome in detail.
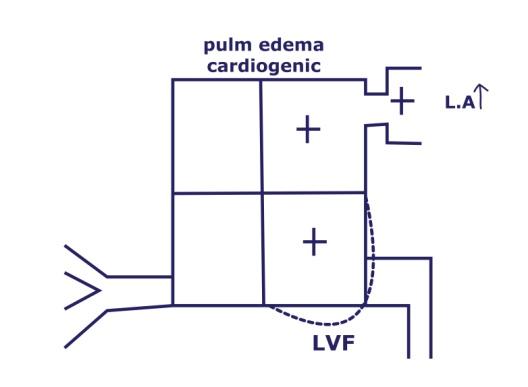
- Cardiogenic pulmonary edema: Increase in left atrial pressure secondary to LVF
- Edematous fluid is transudate
- acute respiratory distress syndrome is due to non-cardiogenic pulmonary edema

Non-Cardiogenic Pulmonary Edema
- Example, A patient has swine flu or bird flu. As the swine flu virus damages pneumocytes without damaging heart, this will end up in ARDS.
- Collapse of alveoli leads to hypoxia and which in turn leads to damage of Endothelium (damage to gap junctions)
- Leakage of fluids from the pulmonary capillary into alveoli
- ARDS occurs in 10% of ICU patients.
- Sudden onset Respiratory distress
- Presence of CXR Bilateral infiltrates on chest X-ray. (no cardiac cause found)
- Reduced pO2 (demonstrable hypoxia)
- Normal left atrial pressure (LAP)
|
Triggers for ARDS |
|
|
Direct (Most common) |
Indirect |
|
|
- Mendelson syndrome: Aspiration of stomach acid (Chemical Pneumonitis)
| Important information Both pneumonia > sepsis are the leading causes of ARDS Leading cause of death after blood transfusion: TRALI Status asthmaticus (disease of the airway) is not ARDS( disease of alveoli) |
Medicine Related Articles:
Clinical Presentation

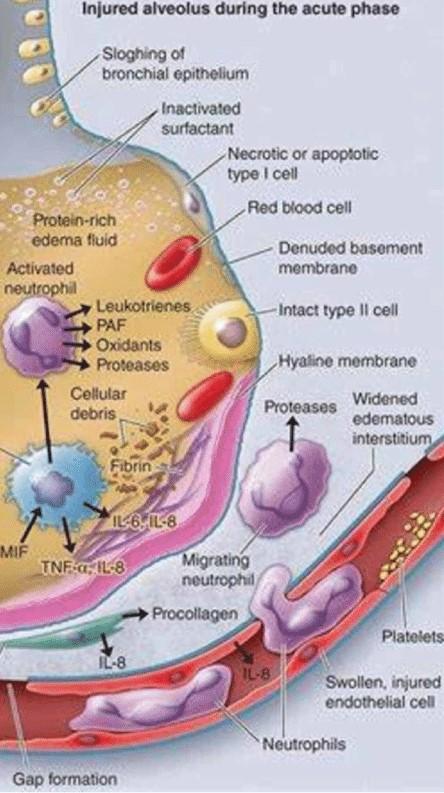
- Type 1 pneumocytes: cover 90% of surface area (injured during adult ARDS)
- Type 2 pneumocytes: produce surfactant (most abundant cell of alveoli)
- IN ARDS, Type 1 pneumocytes are affected, and Type 2 pneumocytes are not affected.
- Normal surfactant with a reduced surface area of alveoli for gas exchange
- Ventilation and perfusion imbalance (perfusion is secondary to the hypoxia component)
- Hypoxia causes dilatation of all blood vessels in the body except vessels of the pulmonary circuit
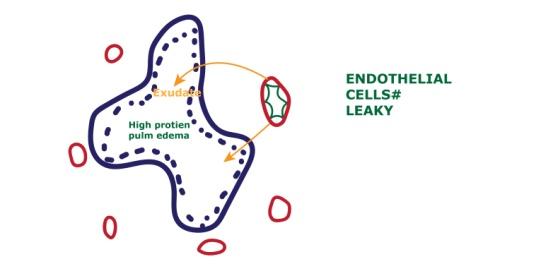
- Most vulnerable cells/most damaged cells in ARDS is endothelial cells of alveoli due to hypoxia
- Endothelial cells become leaky resulting in Exudative high-protein pulmonary edema.
- In heart failure: low protein pulmonary edema
Features: (Sudden onset Respiratory Distress)
|
EXUDATIVE PHASE
|
PROLIFERATIVE PHASE
|
FIBROTIC PHASE
|
- In the initial phase of ARDS, because of tachypnoea, there will be Respiratory alkalosis (CO2 washout)
- In acute asthma: type-1 respiratory failure and respiratory alkalosis due to CO2 washout
- In status asthamaticus: type-2 respiratory failure & Respiratory acidosis due to CO2 overproduction in lungs
- When PCO2 is 60mm of Hg, then the compensatory mechanisms begin to fail.
Work –Up in ARDS
CXR
- In ARDS patient: Bilateral extensive infiltrates
- Cardiothoracic ratio is normal.
- Para cardiac area sparing
- CP angle is normal.
- In cardiogenic pulmonary edema
- Cardiothoracic ratio is increased.
- Bat wing edema seen.
- CP angle is blunted.
- Echo:
- In ARDS: Ejection fraction is normal, LA pressure is normal.
- In cardiogenic pulmonary edema: Decrease ejection fraction and LA pressure increased
- ABG in ARDS: ↓ pO2, ↑ pCO2 (ventilation, perfusion imbalance)
Also Read: EPILEPSY AND Electroencephalography (EEG) : NEET PG Medicine

Essentials of Diagnosis
Sudden onset respiratory distress
- Central line insertion: Pneumothorax
- S. Aureus pneumonia: receiving i.v Vancomycin for 2 days.
- Pneumatocele rupture resulting in Pneumothorax.
- After multiple bone fractures/ Massive blood transfusion or acute pancreatitis.
ARDS: BERLIN Criteria
Sudden onset resp. distress
- CXR: B/L pulmonary infiltrates
- PaO2 / FiO2 < 300 (most important diagnostic criteria for ARDS)
- Absence of left atrial Hypertension
GRADING
ARDS Pa2 / FiO2 Mild
Moderate
Severe<300
<200
<100
- Volutrauma can occur in ARDS: Seen in high or normal volume ventilation resulting in Pneumothorax.
Management of ARDS
Low volume ventilation: 6 ml/kg to minimize BAROTRAUMA to the chest. (Normal tidal volume is 12 ml/kg)
- Plateau pressure of ventilator: <30 cm H2O
- Respiratory rate of ventilator: <35/min
- Prone-position ventilation
- Risk of extubation
- CVP line loss
- Orthopedic injuries
- Extracorporeal membrane oxygenation (ECMO): Patient in whose heart and lungs are too weak for ventilation.

- Limited fluids and diuretics: To maintain normal left atrial pressure.
- Ensure neuromuscular paralysis: Cisatracurium (for effective ventilation)
- Steroids, surfactant therapy and high-frequency jet ventilation (HFJV) have no role in the treatment.
- Most common cause of death in ARDS: Sepsis (non-pulmonary causes)
| Congestive heart failure | ARDS |
| Transudative pulmonary edema | Exudative pulmonary edema |
| Hydrostatic pressure increased | Hydrostatic pressure normal |
| LA pressure increased | LA pressure normal |
| Low protein pulmonary edema | High protein pulmonary edema |
| BNP increased | BNP normal |
And that is everything you need to know about Acute Respiratory Distress Syndrome to boost your Medicine preparation. For more interesting and informative posts like this keep following our blog!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Non-Cardiogenic Pulmonary Edema
Clinical Presentation
Features: (Sudden onset Respiratory Distress)
Work –Up in ARDS
CXR
Essentials of Diagnosis
Sudden onset respiratory distress
ARDS: BERLIN Criteria
GRADING
Management of ARDS
Top searching words
The most popular search terms used by aspirants
- NEET PG Medicine
- NEET PG Strategy
- NEET PG study tips