Emergency Contraception: Overview, Drugs Used, Methods & PYQs
Feb 28, 2023

Emergency contraception refers to the use of contraceptive methods to prevent unintended pregnancy after unprotected sexual intercourse or contraceptive failure. It is an important aspect of reproductive health care, as unintended pregnancies can have significant physical, emotional, and social consequences.
In the NEET PG exam, questions related to emergency contraception may test your knowledge of the different types of emergency contraception, their mechanisms of action, effectiveness, side effects, and contraindications. You may also be asked to identify appropriate candidates for emergency contraception, counsel patients on its use, and manage potential complications.
Read this blog further to learn more about this important OBGYN topic for NEET PG exam preparations.
Overview
- Contraception given to prevent pregnancy, within 72 hours of unprotected intercourse.
- Abortion is not a method of emergency contraception
Important Information
- FSH → Estrogen
- LH → Progesterone
Combined oral contraceptive pills (COCs): Estrogen + Progesterone
↓
Negative feedback to pituitary (no FSH and LH to act on ovary)
↓
Suppresses Estrogen +Progesterone formation by ovary
- COCP causes artificial menstruation in the female.
- Cycles are regular, anovulatory
- Dose of Estrogen is low in COC (Max - 0.03 mg), so it
- Reduces bleeding
- Control anemia
- Since Estrogen is less: Ovarian cancers, endometrial cancers, endometriosis and fibroids are less
Drugs for Emergency Contraception
- Levonorgestrel (LNG): 0.75mgx2 tablets (12 hours apart) now replaced by 1.5 mgx1 Tab
- DOC
- MOA
- ↓Implantation by making endometrium too fluffy
- ↓Tubal motility
- ↓Ovulation (by suppressing LH surge)
- COCP: Yuzpee regimen (outdated) -2 Tab (morning 100ug estrogen) and 2 Tab (evening 100ug)
- MOA
- ↓ ovulation
- ↓ Implantation
- MOA
- Mifepristone: RU 486
- Dose: 25-50 mg
- Antiprogestin
- ↓ Implantation
- IUCD
- Effective upto 5 days of unprotected intercourse
- Most effective method (but not DOC)
Important Information
- Drugs of emergency contraception are not prescription drugs, these are Over the Counter drug
- Ulipristal acetate
- Selective progesterone receptor modulator (SPRM)
- ELLA 30mg
- Equally effective upto 5 days of unprotected intercourse.
Also Read: Amenorrhea: Primary and Secondary
Previous Year Questions
Q. Which of the following is not used as an emergency contraception? (NEET Jan 2020)
A. Danazol
B. Copper T
C. RU 486
D. High dose estrogen
Contraception
IUCD
- 1st generation: Lippes loop (foreign body action)
- 2nd generation: Act by causing aseptic inflammation, spermatotoxic action of copper, foreign body action
- Cu7, Cu 380 Au / Ag (380: Surface area of cu in mm2 on device): Effective for 5 years
- Paragard: Effective upto 10 years
- 3rd generation: Progesterone containing devices
- Progestasert: 38 mg, releasing 65 mcg / day
- LNG devices (MIRENA): 52 mg, releasing 20 mcg / day
- Also used for management of
- Menorrhagia
- Endometriosis
- Endometrial hyperplasia
MOA of IUCD
- Foreign body action
- Endometrium non receptive
- ↓↓ Ovulation
Important Information
- Progestasert is having another action: Act by thickening of cervical mucous (main action); LNG also makes cervical mucosa thick but main action is making endometrium non - receptive
Also Read: Endometrial Carcinoma (Endometrial Hyperplasia's, Staging Of Ca Endometrium)
Side Effects of IUCD
- M/C: Bleeding (3 x) > Pain
- Perforation at insertion
Important Information
- For first three months: For bleeding after IUCD we give prophylactically NSAIDS and Tranexamic acid to some patients
Pregnancy with IUCD in situ
- Management
- If patient wants to abort: MTP
- If patient wants to continue: Remove IUCD; if thread is not visible then explain that there are 50 % chances of abortion
Important Information
- Overall chances of ectopic pregnancy are slightly more with patient having IUCD as compared to normal women having pregnancy
Lost IUCD
- First step: Exploration in OPD with artery forceps
- If not found then do USG and locate device
↓ if not found
Radiography (X - ray): Rule out pregnancy first beforehand
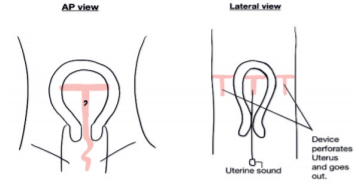
- In lateral view if the Uterine sound and copper device are in same plane: Copper T is inside.
Also Read: Molar Pregnancy and Gestational Trophoblastic Disease - NEET PG OBGYN
.jpg)
Sterilization
Vasectomy
- Failure rate < 0.1 %
- Non scalpel vasectomy: Done by artery forceps under local anesthesia
- Avoid intercourse without condoms / barriers for 3 months or till 30 ejaculations.
- After 3 months: Semen analysis is done to see Azoospermia.
- Reversibility is only 30-35 % successful (Vaso vasal reanastomosis)
Tubectomy
- Puerperal Tubectomy
- Within first 7-10 days (best done 2-3 days from delivery)
- Done by open technique: Mini laparotomy (1.5-2 inches incision)
- Interval sterilization: After 6 weeks; mostly done by laparoscopy
- Concurrent sterilization: Done along with another surgery (LSCS + T/L, MTP + T/L)
- Site of ligation: Isthmus
- Reanastomosis of Tubectomy (reversibility)
- Isthmo isthmic reanastomosis: Upto 80 % successful (uniform cut ends)
- Isthmo-Ampullary Reanastomosis: 30 % successful
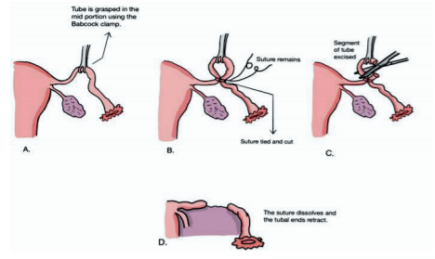
- M/C method for tubectomy: Modified Pomeroy's method: Risk of spontaneous Reanastomosis
- Other methods
- Parkland’s Technique
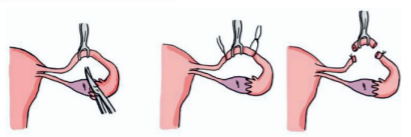
-
- Irwing surgery Technique: We cut the tube and bury into uterus and the other end buried into mesosalpinx; failure rate is very less
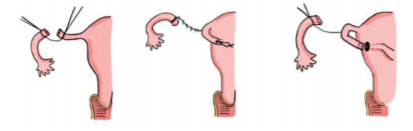
-
- Kroners: Fimbriectomy; not done nowadays
- Madlener’s method: Only crushing of tube done; no cutting, so high failure rate, so not done.
- Essure ring
- Hysteroscopic procedure; putting of Nitinol (Nickel + Titanium) coil into tube; causes fibrosis of the interstitial part of tube within 3 months.
- Hysterosalpingography is done after 3 months to confirm the fibrosis
Also Read : Genital Warts: Causes, Symptoms, Risk Factors, Diagnosis, Treatment and Complications
Failure Rates Of Contraceptives
- Failure rate of contraception drugs is calculated by PEARL INDEX (total number of accidental pregnancies/ total months of exposure) x 1200
- Rates of failures
- Vasectomy: 0.1%
- Tubectomy: 0.2%
- IUCD: 0.5-0.6% (copper devices); 0.2% (Levonorgestrel)
- Combined OCPs: 0.6-0.7%
- Progesterone Only pill: 1 -2%.
- Barrier methods (male): 14 -20 %
- Natural method: Worst
- Implants like Norplant, implanon: 0.05%
Progesterone Implants
- Norplant: 6 stems (36 mg each =216 mg of LNG); Applied as subdermal implant over the arm; effective till 5 yrs.
- Norplant-2 / JADELLE: 75mg x2 = 150 mg of LNG (2 stems); effective for 5 years
- Etonorgestrel implants: Synthetic / degradation product of desogestrel and extremely effective
- Implanon: 68 mg single stem effective till 3 years; withdrawn in most countries
- Nexplanon: Ba coated; radiopaque implant so easy to locate & remove later on
COCPs
- E + P ? inhibits FSH and LH from pituitary
↓
Ovary suppressed
- Estrogen causes proliferation of uterus
- Progesterone cause secretion of endometrium
- So, women will have artificial periods
- Women do not ovulate & do not conceive
- MALA - D, MALA - N
- Estrogen: 0.03 mg (30 µg)
- Progesterone: 0.15 mg (150ug)
Also Read: How to Prepare Gynaecology and Obstetrics for Medical PG Entrance exams?
Natural Methods Of Contraception
- Failures 60 / 100 WY
Calendar/ Rhythm/ safe period or fertile period method
- From 11 -16th day: High chance of conception as on 14th day ovulation occurs
- So, avoid sex in this period
Cervical mucus method
- Watery mucus occurs during ovulation period
- Causes wetness in vagina
- Avoid intercourse in this period
- Known as Billing's method
Also Read: Spontaneous and Induced Abortions - NEET PG OBGYN
Withdrawal method
Basal body temp
- Increases during ovulation, progesterone is a thermogenic hormone
Previous Year Questions
Q. A woman with an IUCD came to OPD for removal but the Gynecologist could not remove the IUCD as there was no thread visible to pull on. To locate the lUCD an Ultrasound was done. The IUCD was seen besides the ovary. How would one remove this IUCD? (FMGE June 2021)
A. Hysteroscopy
B. USG guided removal by an IUCD hook
C. Laparoscopy
D. Laparotomy
Q. The oral contraceptive pill 'Mala N' contains which of the following type of progesterone component? (JIPMER Dec 2019)
A. Levonorgestrel
B. Etonorgestrel
C. Desogestrel
D. Drospirenone
Q. Which of the following is not a mechanism of action for oral contraceptive pills? (AIIMS 2020)
A. Prevents ovulation
B. Prevents Implantation
C. Thickens Cervical mucus
D. Increases gonadotropin secretion
To study this topic in detail, download the PrepLadder app and find in-depth video lectures by India’s top OBGYN faculty.
Also Read: Important Topics in OBGYN for NEET-PG by Dr. Prassan Vij

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Overview
Drugs for Emergency Contraception
Previous Year Questions
Q. Which of the following is not used as an emergency contraception? (NEET Jan 2020)
Contraception
IUCD
MOA of IUCD
Side Effects of IUCD
Pregnancy with IUCD in situ
Lost IUCD
Sterilization
Vasectomy
Tubectomy
Failure Rates Of Contraceptives
Progesterone Implants
COCPs
Natural Methods Of Contraception
Calendar/ Rhythm/ safe period or fertile period method
Cervical mucus method
Withdrawal method
Basal body temp
Previous Year Questions
Q. A woman with an IUCD came to OPD for removal but the Gynecologist could not remove the IUCD as there was no thread visible to pull on. To locate the lUCD an Ultrasound was done. The IUCD was seen besides the ovary. How would one remove this IUCD? (FMGE June 2021)
Q. The oral contraceptive pill 'Mala N' contains which of the following type of progesterone component? (JIPMER Dec 2019)
Q. Which of the following is not a mechanism of action for oral contraceptive pills? (AIIMS 2020)
Top searching words
The most popular search terms used by aspirants
- NEET PG OBGYN
- NEET PG Strategy
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial