Nephritic Syndrome And Nephrotic Syndrome
Feb 16, 2023

Nephritic syndrome is a common cause of acute kidney injury and is seen in a variety of underlying diseases such as glomerulonephritis, lupus nephritis, and IgA nephropathy. It can lead to rapid decline in kidney function, and early recognition and treatment are crucial to prevent permanent kidney damage and progression to chronic kidney disease.
Therefore, understanding the pathogenesis of nephritic syndrome is important in order to understand the underlying mechanisms of kidney injury and develop appropriate treatments.
Let's learn about this commonly tested Pathology topic for the NEET PG exam preparation.

Post Streptococcal Glomerulo-Nephritis
- M.C cause of nephritic syndrome in pediatric age group. It occurs 14 days after skin or throat infection. It is characterized by antigen-antibody complex formation (type 3 hypersensitivity reaction). Clinical features: Cola coloured urine, sore throat 14 days prior to this
Microscopic findings
- All the glomeruli are affected. Presence of increased cellularity of glomerulus (diffuse hypercellularity)
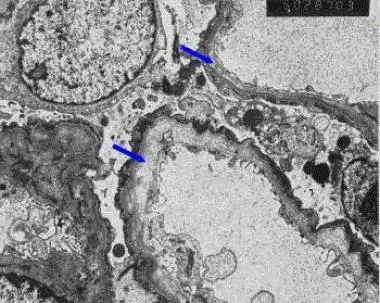
Electron microscopic examination
- Presence immune complexes (Type III hyper sensitivity). Immune complexes are deposited in sub-epithelial areas known as subepithelial hump
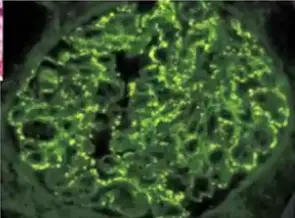
- Immunofluorescence: Granular appearance/starry sky appearance.
|
Important information Various starry sky appearances
|
RPGN (Rapidly Progressive Glomerulonephritis)/ Crescentic GlomeruloNephritis
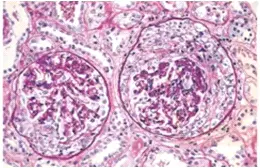
- There is increased proliferation of parietal epithelial cells and infiltration of monocytes, neutrophils and deposition of fibrin in glomeruli (Responsible for formation of crescent)
- Rapid proliferation results in decline in kidney function in a short duration of time.
- It is of following 3 types
- Anti GBM antibody disease/ Goodpasture syndrome.
- Immune complex disease e.g. SLE
- Pauci-immune disease – It is associated with vasculitis disorder like Wegener’s glomerulonephritis
- More the number of the crescents in glomeruli, more is the severity of disease.
FLEA-BITTEN KIDNEY
- It is seen in
- Malignant hypertension
- PSGN
- Vasculitis disorder
- Infective endocarditis
- Immune complex forming disorders like leukemia and lymphoma.
Berger Disease / IgA Nephropathy

- Most common cause of glomerulonephritis in adults. It occurs 2-3 days after sore-throat / upper respiratory tract infection. Abnormal IgA antibodies are deposited in mesangial cells. Mesangial cells have CD71 receptors
- Biopsy finding with immunofluorescence:
- Shiny yellow green appearance of material
- Confirm immune complexes in mesangium
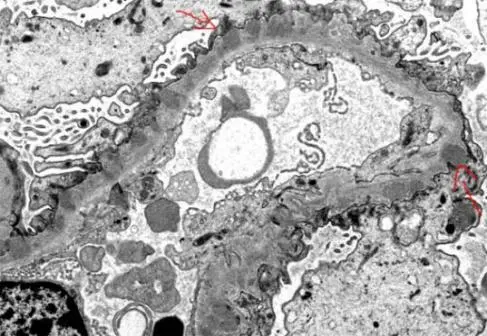
Alport Syndrome
- There is a defect in a 5 chain of collagen type IV (note: a 4 chain of college is defective in familial hematuria).
- Presence of abnormal thickening, there will be variations in the thickness of basement membrane (at some places basement membrane is thick and other places it is thin) causing splitting of lamination in basement membrane, this kind of variation in thickness is called “basket weave appearance”. This is seen in electron microscopy.
|
Important Information
|
Granular Vs. Linear immunofluorescence
|
Linear IF |
Granular IF |
|
|
|
|
|
|

Also Read:
NEPHROTIC SYNDROME


Minimal Change Disease
- Most common cause of nephrotic syndrome in children, especially 2-6 years of age.
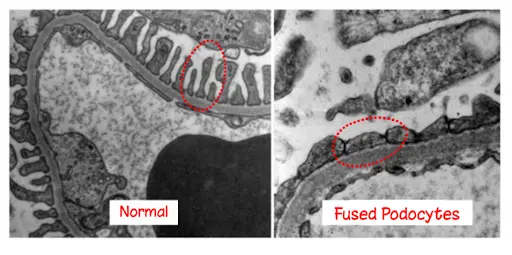
Clinical features
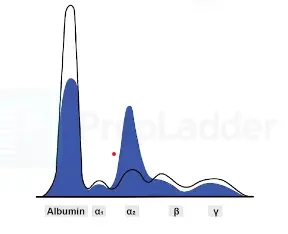
- Generalized Edema (it occurs due to excessive salt and water and hypoalbuminemia). Massive Proteinuria occurs resulting in frothiness of urine. It is characterized by selective proteinuria. Therefore, patients have a very good response to steroids. Under light microscopy no abnormality is detected.
|
Important Information
|
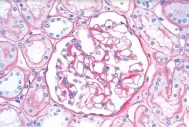
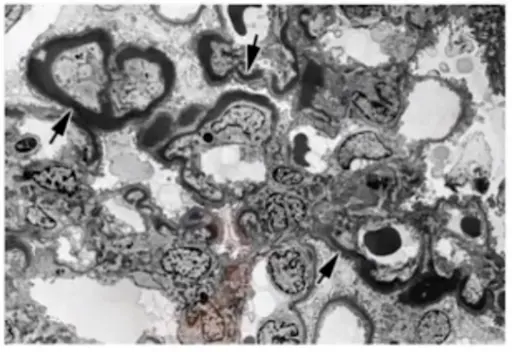
Membranous Glomerulopathy

- It is the most common cause of nephrotic syndrome in elderly patients.
- Etiology
- Idiopathic(In idiopathic variant , antibodies are formed against phospholipase A2 receptor)
- Solid malignancy
- Connective tissue disorders
- Infections
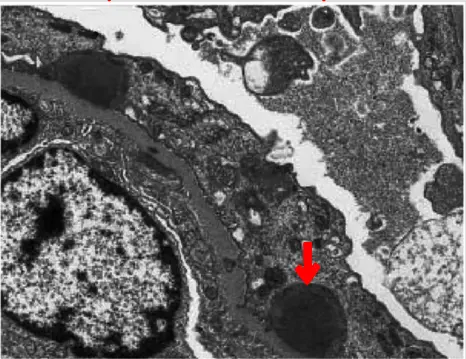
- This condition is characterized by Subepithelial immune complex deposition. On electron microscope: it appears as black electron dense deposits in the subepithelial region giving SPIKE and DOME appearance. On immunofluorescence: granular deposits are seen.
- Membranous glomerulopathy is an important cause of Non-selective proteinuria. So steroids alone are not sufficient in these patients. along with steroids cyclosporine is also given. Animals model: HEYMANN NEPHRITIS model. Rat kidney antigen used is Megalin
Focal Segmental Glomerulosclerosis
- It is the most common cause of nephrotic syndrome in adults. It is associated with HIV infection, single kidney and sickle cell anemia. Worst prognosis: collapsing variant as it is associated with HIV. Best prognosis: glomerular Tip type
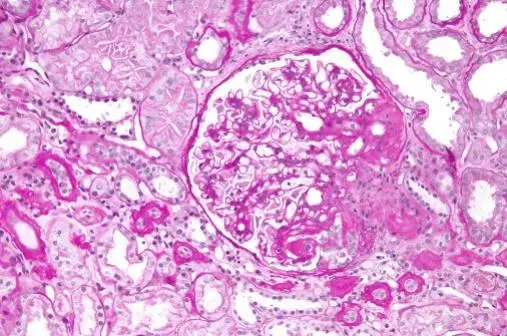
MPGN Type I
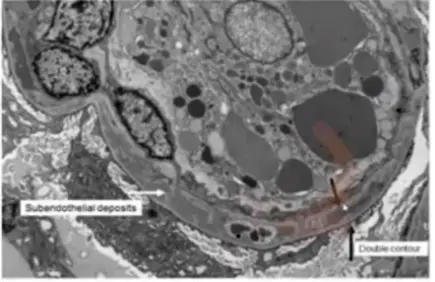

- MPGN- membranoproliferative glomerulonephritis is also called Measangio-capillary glomerulonephritis. Characterized by thickening of basement membrane and subendothelial deposits. Basement membrane material covers Subendothelial Deposit on both sides. This is responsible for “Tram-Track appearance of basement membrane “
MPGN Type II
- Due to deposition of amorphous electron dense material in basement membrane k/as dense deposit disease. Specific antibody: C3 nephritic factor
To learn this important Pathology topic in detail, download the PrepLadder app and discover excellent video lectures by a subject matter expert.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Post Streptococcal Glomerulo-Nephritis
RPGN (Rapidly Progressive Glomerulonephritis)/ Crescentic GlomeruloNephritis
Berger Disease / IgA Nephropathy
Alport Syndrome
Granular Vs. Linear immunofluorescence
NEPHROTIC SYNDROME
Minimal Change Disease
Clinical features
Membranous Glomerulopathy
Focal Segmental Glomerulosclerosis
MPGN Type I
MPGN Type II
Top searching words
The most popular search terms used by aspirants
- NEET PG Pathology