Burn Resuscitation And Management
Apr 6, 2023

Any injury to the skin or any other organic tissue that is primarily caused by heat, radiation, radioactivity, electricity, friction or through chemical contact is called a burn.
Burns are an essential topic for your Surgery preparation. Read this post thoroughly to understand everything you need to understand about Burns.

Burns
Indications of Referral to Dedicated Burn Center
Partial thickness burn involving > 10% of TBSA
- Any full thickness burns
- Burns involving face, hands, foot, joints and genitalia.
- Electrical burn
- Chemical burn
- Burn with inhalation injury
- Burn with trauma
- Burn with comorbidity in elderly
- Burn in children requiring special emotional care
Pathophysiology
- ↑ Radiant loss: Secondary to ↑ blood flow & integumentary loss
- Heat loss: Evaporation of water from burn wound (also cause fluid loss)
- Massive release of inflammatory mediators: leads to
- Vasodilation
- ↑ Capillary permeability – Extravastation of fluid - Edema- third space fluid loss- hypovolemia
- Global depression of immune function
- Release of Catecholamines, Glucagon, Corticosteriods → Hypermetabolism → Fever
- Curling ulcers
- It is a stress ulcer that occurs only when 1/3rd of TBSA is burnt.
- Caused due to ↓ decreased mucosal defenses due to hypovolemia (Acid secretion in stomach is normal)
- Occurs due to increased acid secretion.
Important Information
In patients of head injury
Has stress Ulcer knowns as Cushing ulcers
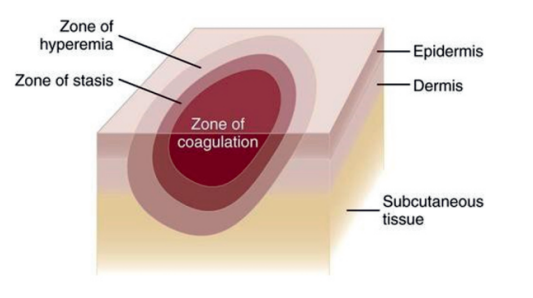
Areas of Cutaneous injury in Burn
|
Zone of coagulation |
Zone of stasis |
Zone of hyperemia |
|
|
|
Important Information
- Best temperature of water used for cooling of burn wound 15ºC
- Cold water or Ice shouldnot be used as it causes vasoconstriction leading to ↓ tissue perfusion
Burn Classification (Based on Depth Burn)
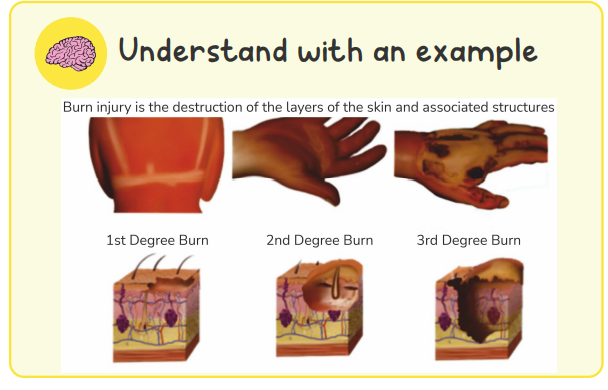
First Degree Burns
- Aka Epidermal burn
- Only epidermis is involved
- Painful & erythematous
- No blisters formation
- Healing occurs without scarring within 5-10 days
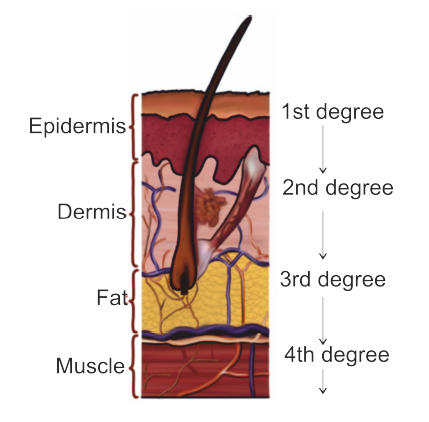
Second Degree Burns
- Aka Partial thickness burn
- It is divided into
|
Superficial partial thickness burn |
Deep partial thickness burn |
|
|
|
|
|
|
|
|
Third Degree Burns
- Aka full thickness burn
- Involvement of Epidermis + dermis + Subcutaneous fat
- Burn surface has black colored leathery circumferential eschar – Escharotomy is done to prevent compartment syndrome.
Characteristic features:
- No pain, no blisters, no pin prick sensation
- Healing occurs with contracture: To prevent contracture -
Excision of burned skin with skin grafting after resuscitation if the patient.
Fourth degree Burn
- Involvement of Skin + underlying structures (Muscle, bone & brain)
Surgery Related Articles:
Causes of Death in burns
- MC cause of death at the site of burn: Asphyxia
- MC cause of early death in burns: Hypovolemia / shock
- MC cause of late death in burns: Sepsis
- Overall MC cause of death in burns: Sepsis
- MC organism responsible for sepsis in burns: Pseudomonas
Danger Signs of Airway Burns
Burns involving head, neck & face
- Singed / burned nasal hair
- Carbonaceous deposits in the sputum
- Hoarseness of voice
- H/o burns in a closed room
Important Information
- In all this patient’s Elective intubation is the safest
- Delay in intubation leads to Laryngeal edema → difficulty in intubation – Emergency Cricothyroidotomy should be performed.

Management of Burn Patient
Fluid Resuscitation
- Venous access in adults
- Ideal sites: Veins of Hand, Antecubital fossa or neck
- Saphenous vein cut down
- Performed during difficult accessibility
- Preferred over Central line insertion
IV Fluid Resuscitation

- Fluid of choice: Ringers lactate
- Maintenance fluid of choice in children: Dextrose normal saline (DNS) as children have lesser glycogen storage
- Other fluids used are
- Hypertonic saline
- Normal saline
- Fresh frozen plasma
- Human Albumin
- Hypertonic saline is used for burn shock patients as it has higher oncotic pressure and will be retained in vascular compartment.
Calculation for fluid requirement
Parkland Formula
- It is Crystalloid based
- 24 hrs. fluid requirement = 4 ml × body weight (kg) × % of burned surface area
- Time starts when the patient gets burned
- First degree burns are not included
- Maximum fluid given should be taken for 50% TBSA- to avoid fluid overload
- Half of calculated fluid is given in first 8 hours and rest half of fluid is given in next 16 hours.
- 2nd day fluid requirement should be 40-60% of first day fluid requirement.
ATLS modification of Parkland formula
- It is based on
- Age
- Weight
- Type of injury
- Adults, children ≥ 14 years
- 2 ml × body weight × % BSA
- Children <14 years, ≤30 kg weight
- 3ml × body weight × % BSA
- Electrical burns (irrespective of age)
- 4ml × body weight × % BSA
|
Burn resuscitation fluid rates and Target Urine output by Burn type and Age |
|||
|
Category of Burn |
Age and Weight |
Adjusted Fluid rates |
Urine Output |
|
Flame or Scald |
Adult and older 14 children (>_14 years old) |
2 ml LR × kg × % TBSA |
0.5 ml / kg/hr 30-50 ml/kg/hr |
|
Children (<14 years old) |
3 ml LR × Kg × % TBSA |
1 ml / kg / hr |
|
|
Infant and young children (£ 30 kg) |
3 ml LR × kg / % TBSA Plus a sugar – containing solution at maintenance rate |
1 ml/kg/hr |
|
|
Electrical injury |
All ages |
4 ml LR x Kg x % TBSA until urine clears |
1-1.5 ml/ kg / hr until urine clears |
|
LR: Lactated Ringer’s solution TBSA: Total Body Surface Area |
|||
Brooke Formula
- Both Crystalloid & Colloid based
- Fluid requirement = 1.5 ml/ kg/ % TBSA of crystalloids + 0.5 ml/kg/% TBSA of Colloids + 2 liters of free water
Galveston
- It is a Pediatric formula
- Fluid requirement = 5000 ml/m2 of total burned surface area + 1500 ml/m2 of Total body surface area
Monitoring of fluid resuscitation
- Best clinical indicator of tissue perfusion: Urine output
- Minimum U.O. after adequate tissue perfusion in adults: 1ml/min
- Minimum U.O after adequate tissue perfusion in children: 0.5-1.0 ml/min
- In patients of Cardiac dysfunction monitoring is done by
- Trans – Esophageal USG (or)
- Central line
Estimation of burn surface area
Determination of burn size – estimates the extent of injury
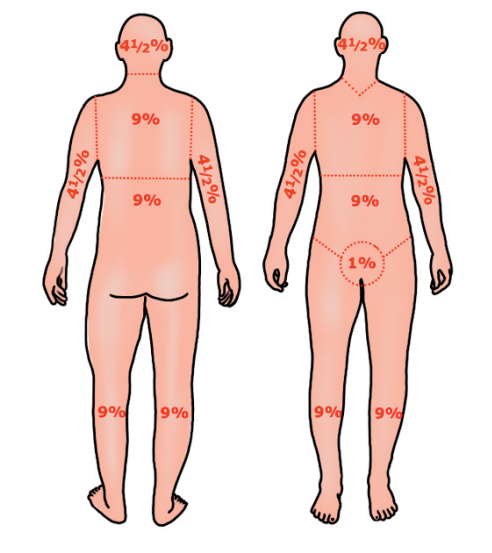
Rule of “9”
- Given by Alfred Russel Wallace
- Rule of 9 is followed for adults but is not very accurate for children
- In case of children limbs are 14 percent each
Lund & Browder chart
- More accurate for estimation of burn surface area in Children
Berkow’s formula
- Also used for estimation of burn surface area in Children
Palmar method
- For estimation of smaller patchy burns:
- Area of Open hand - Accounts for 1%
- Used for
- Splash burns
- Mixed distribution of burns
Care of burns patient
Cool the burn wounds
- Uses
- Provides analgesia
- Slows the delayed microvascular damage
- Cooling should be done for a minimum of 10 mins
- Cooling is effective upto 1 hr after burns
- Best temperature of water used for cooling of burn wound 15º C
- Tap water can also be used
- Cold water or Ice should not be used because it increases the risk of Hypothermia
- Cutaneous vasoconstriction; Extend the thermal damage
- Superficial partial thickness burns
- Heals without scarring within 2 weeks
- Exposure method can be used – given Antimicrobial without dressing
- Escharotomy
- Performed for circumferential eschar
- Layers incised are longitudinally
- Skin
- Superficial fascia
- Deep fascia
Management of burn wounds
Exposure method
- No dressing is done
- Antimicrobials given 2-3 times / day
- Used for burns in Face & Head
Disadvantages
- Increased pain & heat loss
- Increased risk of cross – contamination
- Closed method
- Occlusive dressing is applied over Antimicrobial agent
- Changed twice daily
Advantages
- Decreased Pain & heat loss
- Decreased risk of cross- contamination
Disadvantages
- Increased risk of bacterial growth – if dressing is not changed twice daily
- Topical antimicrobials
- Silver sulphadiazine (1%)
- Provides Broad spectrum anti – microbial prophylaxis – mainly against Pseudomonas & MRSA
- Silver nitrate (0.5%)
- Highly effective against Pseudomonas colonization
- Causes “Black staining” of furniture around patients
- Mafenide acetate (5%)
- Used in USA
- Painful to apply
- Usage is associated with Metabolic acidosis
- Silver sulphadiazine & Cerium nitrate
- Used for full thickness burns
- Induces hard effect on burned skin
- Mainly used in elderly: Increases cell mediated immune suppression (CMI) - Cerium nitrate
- Forms sterile eschar
- Boost CMI
- Dressing materials
- Alginate
- Absorptive, but non – adherent
- Used in high drainage wounds
- Foam
- Can absorb moderate or heavy exudate
- Used for high – drainage wounds
- Contraindicated in non – draining wounds
- Hydrocolloid
- Facilitate Autolytic debridement – used for Bedsores & stasis ulcers
- Not used in high drainage wounds
- Hydrogel
- Rehydrates the wound bed
- Facilitate Autolytic debridement
- May macerate the wound by over – rehydration
- Transparent film
- Non – absorptive
- Facilitate Autolytic debridement
- Not used in high drainage wounds
- Alginate
Management of Chemical Burn
- Copious irrigation with water or saline
- Performed for a minimum of 20 minutes
- Exceptions
- Elemental metals: Causes exothermic reaction with water
- Phenol: Leads to deeper infiltration of tissues
- Treatment should continue – until skin pH is normal
- Remove the contaminated clothing & jewellery
- Do not try to neutralize the chemical burn
- Neutralization causes Exothermic reaction – leads to further injury
Also Read :
Electrical Injury
In Direct current (DC)
- It is low tension / Electrical appliances injury
- It does not have enough energy to cause extensive tissue destruction
- Because of increased resistance – Cause small deep burn at the site of entry & exit → fingers & toes
- Tendon & Nerve damage can occur
In Alternate current (AC)
- Creates tetany in the muscle: Patient can’t detach from device until main power is turned off
- Main danger: AC interferes with normal cardiac pacing without causing significant Myocardial damage, ECG is done
Q. Al of the following are correct about management and complications of burn except
- M/C cause of death is sepsis
- Exposure method is used for face and hand
- Silver sulphadiazine is effective against pseudomonas and MRSA
- Galveston formula is colloid base
Q. Which of the following patient should be referred to designated burn center for the management?
- Burns involving the face, hand, feet, genitalia, perineum or major joints
- Any full thickness burn
- Electrical injury including lightning injury
- All of the above
Q. Match the following
|
|
- I-E; 2-A; C:3- B, D
- I-D; E; 2-A; C:3- B
- I-D; E; 2 A; 3- B, C
- I-E; 2-A; D:3- B, C
Q. Match the following
|
|
- I-A, F; 2-A, C, F; 3-B;4-D, E; 5-B, G
- I-A, 2-A, C, F; 3-B; 4-B, D, E; 5-B, G
- I-A, F; 2- C, F; 3-B; 4-B, D, E, 5-B, G
- I-A, F; 2-A, C, F; 3-B; 4-B, D, E; 5-B, G
Q. A 50 year old female with 50 kg body weight suffered from burns after pressure coocker blast, involving 60% of total body surface area, how much fluid should be given in first 8 hr ?
A. 4L
B. 5L
C. 6L
D. 7L
Q. In the above ques. Calculate the second day fluid requirement?
A. 5L
B. 8L
C. 10L
D. 12L
Q. All of the following are correct about estimation of burn size except
- In infant head and neck corresponds to 21% and each leg 13%
- Lund and Browder chart is preferred over berkow formula for accurate determination of burn size in children
- Area of open hand is helpful in evaluating splash burns and burns of mixed distribution
- Area of open hand include the area under the palm approximately 1% of TBSA.
And that is everything you need to know about Burns for your Surgery preparation. For more interesting and informative blog posts like this, download the PrepLadder App and keep following our blog.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Burns
Indications of Referral to Dedicated Burn Center
Pathophysiology
Areas of Cutaneous injury in Burn
Burn Classification (Based on Depth Burn)
First Degree Burns
Second Degree Burns
Third Degree Burns
Fourth degree Burn
Causes of Death in burns
Danger Signs of Airway Burns
Management of Burn Patient
Fluid Resuscitation
IV Fluid Resuscitation
Calculation for fluid requirement
Parkland Formula
ATLS modification of Parkland formula
Brooke Formula
Galveston
Monitoring of fluid resuscitation
Estimation of burn surface area
Lund & Browder chart
Berkow’s formula
Palmar method
Care of burns patient
Cool the burn wounds
Management of burn wounds
Exposure method
Disadvantages
Advantages
Disadvantages
Management of Chemical Burn
Electrical Injury
In Direct current (DC)
In Alternate current (AC)
Q. Al of the following are correct about management and complications of burn except
Q. Which of the following patient should be referred to designated burn center for the management?
Q. Match the following
Q. A 50 year old female with 50 kg body weight suffered from burns after pressure coocker blast, involving 60% of total body surface area, how much fluid should be given in first 8 hr ?
Q. In the above ques. Calculate the second day fluid requirement?
Q. All of the following are correct about estimation of burn size except
Top searching words
The most popular search terms used by aspirants
- NEET PG Preparation
- NEET PG Strategy
- NEET PG Surgery