Aneuploidies Including Turner And Klinefelter Syndrome
Nov 3, 2023

Turner Syndrome
- It is a syndrome that is characterized by the monosomy of X CHROMOSOME and has a very characteristic phenotype. There is a loss of one X chromosome, and therefore they are always female.
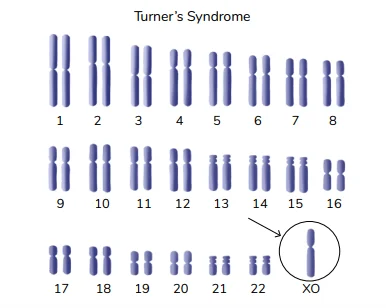
- It can be seen from the diagram that there is a single X chromosome with the other counterpart missing. This is what Turner syndrome will look like.
Incidence And Cytogenetics
- The incidence is 1 in 2500 live births to 1 in 5000 live births. It is a fairly common genetic disorder. The percentage of fetuses aborted in the uterus is greater than 95%. Most of these patients are found to have 45 XO as their genotype. In 75% of the cases, the missing sex chromosome is of paternal origin. This condition is not associated with advanced maternal age. Other cytogenetics that can produce Turner syndrome include Mosaicism. Mosaics usually have a variable presentation (some features are normal, and some are not). One form is 45XO/46 XX. Another form of mosaicism that can be seen is 45 XO/46 XY. Due to the presence of the Y chromosome, there may be features of virilization. These patients also tend to develop malignancies of the gonads (gonadoblastoma). Isochromosomes are another rare manifestation. These are chromosomal abnormalities where the division of chromosomes happens horizontally. The 2p arms are lost. The other two arms have 2q copies. These copies tend to exist as a normal structure (46, X i(qx)).
Clinical Features
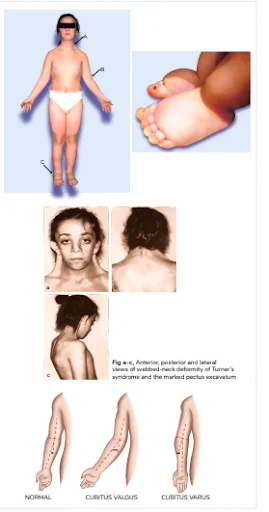
- In the neonatal period, some of these children may appear to be normal while others might have manifestations (small for gestation age, webbed neck, and a hallmark feature of congenital dorsal lymphedema of hands and feet- called the soft neonatal marker).
Adults And Children
- The female will have short stature (less than 145 cm in adults), she will have a short webbed neck which is a remanent of intrauterine cystic hygroma, widely spaced nipples, there is cubitus valgus elbows in the patients, and dorsal lymphedema. The patients have low posterior hairlines. The patients have a shield-like chest that is associated with widely spaced hypoplastic nipples. The specials have bony abnormalities, such as scoliosis, and an increased carrying angle at the elbow called cubitus valgus. These children have short fourth metacarpals and metatarsals. These children have Madelung deformity. Renal abnormalities are found in 60% of the cases, and the most common renal abnormality is the horseshoe kidney. Sometimes there might also be renal pelvic abnormalities. Cardiovascular abnormality for seen in about 40% of the cases (bicuspid aortic valve being the most common, followed by the coarctation of the aorta followed by aortic stenosis). There are cardiac conduction defects in this condition. Increased dislocation of the hip and increased patellar dislocation can be seen in this condition. Multiple pigmented naevi of the skin and cystic hygromas are often a feature. A high-arched palette is also seen as a feature. The patients may also have persistent dorsal lymphedema.
Gonadal Dysgenesis
- In this, ovaries are replaced by fibrous fatty tissues. Streak gonads or streak ovaries are a feature of this condition. These produced primary amenorrhea (high serum FSH levels and serum LH levels). There is an absence of secondary sexual characteristics. There is the presence of a hypoplastic uterus. The person is sterile in such a condition.
Increase Risks
- There is an increased risk of the development of the following conditions. Type 2 diabetes mellitus, Celiac disease, Autoimmune hypothyroidism, Inflammatory bowel disease, Recurrent otitis media and SNHL, Gonadoblastoma- in Turner syndrome Mosaics having Y chromosome or its remnants, Subtle eye abnormalities - Red Green color blindness, Cataracts, Strabismus.

Also Read: Infections of the Upper Airway- Common Cold and Sinusitis
Management Of Turner Syndrome
- Growth hormone therapy is a form of management that can increase the patient's stature by 10 to 15 cm. If the patient is found to be suffering from hypothyroidism, thyroxine is replaced. After 10 years of age, regular thyroid screening is recommended in the patients. Ovarian hormone replacement is also a form of management (either with conjugated estrogen ( 0.3 mg/dl) or with ethenyl estradiol (EE2) 5-10 microgram/day , starting at 14 years of age). After that, the patient should be (after the completion of 6 to 12 months) started on cyclic estrogen and progesterone. Prophylactic gonadectomy can be done in those with any Y chromosomes due to mosaicism.
These patients may have specific learning disabilities, although the patient's cognition may be normal (normal IQ). 70% of the patients have learning disabilities and are sometimes found to have awkward social behaviour and clumsy or fidgety nature while public dealing.
Also Read: KAWASAKI DISEASE : History, Symptoms, Causes and Treatment
Antenatal Diagnosis Of Turner Syndrome
- The following features are seen in the foetus with Turner syndrome. First Trimester: Increased Nuchal Translucency. Second Trimester: Cystic hygroma or generalized hydrops. Confirmation can be done by Karyotype, and the sample may be obtained by CVS/Amniocentesis/Cordocentesis. The risk of recurrence is less than one per cent.
Q1. What are the most consistent features of Turner Syndrome?
- Growth failure is seen in 50 to 90% of the cases, and streak gonads can lead to infertility.
Q2. Which variety of Turner syndrome is associated with low IQ?
- Isochromosome causing Turner syndrome.
Q3. Before 12 years of age, no estrogen or progesterone should be given.
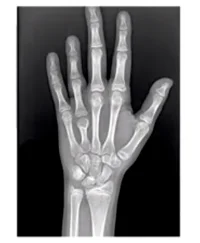
- There is a short 4th metacarpal in the MCQ visual given above, also known as the metacarpal sign. It is a common feature of Turner syndrome.
Also Read: The Genetics of Down Syndrome
Differential Diagnosis Of Turner Syndrome: Noonan Syndrome
- Earlier, it was known as the pseudo-Turner syndrome. A person suffering from this syndrome will have a webbed neck, short stature, increased carrying angle of elbows, and hypogonadism. This syndrome is not a chromosomal disorder. This is a gene-related defect. The PTPN-11 gene, which also shows autosomal dominant inheritance, is responsible for most cases of this syndrome. This can occur in both males and females. There is no occurrence of streak gonads in this syndrome. A patient having this syndrome shows anti mongoloid slant of eyes. This syndrome shows a different congenital heart disease (pulmonary stenosis).
Klinefelter Syndrome
- According to Nelson's 21st edition, It is the most common cause of hypogonadism and infertility in males. It is the most common sex chromosome aneuploidy in humans.
Cytogenetics
- The most common cytogenetic abnormality (in 80% of the cases) is 47, XXY. The extra X chromosome is responsible for the syndrome. This happens due to the non-disjunction of chromosomes during meiosis 1. In 54% of the cases, it is maternal; in 46% of the cases, it is paternal. This syndrome shows an association with advanced maternal age and possible paternal age. Other genetic abnormalities leading to the syndrome. Severe Aneuploidies- In this case, the number of X chromosomes is even larger, and therefore it can be understood that the more the number of X chromosomes, the more severe the manifestation. Some patients with mosaicism may also develop the syndrome.
Also Read: Pigmentary Disorders in Children
.png)
Prevalence Of Klinefelter Syndrome
- It is usually said that the prevalence of the syndrome is 1 in 1000 live births. According to Nelson's 21st edition, the prevalence of the syndrome is increasing now, with the prevalence being 1 in 580 live births. Possibly the reason is deemed to be related to environmental influences on spermatogenesis. The proportion of cases due to paternal non-disjunction is rising.
Clinical Features

- They may appear normal and remain undiagnosed in the first 10 to 12 years. The symptoms come to attention around the time of puberty. The growth of penis ,testis and secondary sexual characters is very slow and is usually a marker for this syndrome. These children have short stature, decreased body hair, small penis, small testis, some may have undescended testis. They usually have lower IQs, but they are not severely mentally retarded. For every X chromosome, the IQ falls by 10 to 15 points. The specials lie at risk of developing specific learning disabilities. They have particular problems relating to verbal commands and their cognitive abilities. These patients are infertile. Small testicles are seen in the patients.
Increased Risks Associated With This Syndrome
- The patients lie at an increased risk of developing type 2 Diabetes mellitus. The patients lie at an increased risk of developing metabolic syndromes. SLE and other autoimmune diseases are common in these patients. These patients are at a 20 times higher risk of developing male breast cancer. Extragonadal germ cell tumours, mediastinal being the most common location. The patients lie at an increased risk of developing Mitral Valve Prolapse.
Investigations
- Many of these patients remain undiagnosed throughout their lives. In infancy, it is seen that the testosterone level is slightly low. Normal AMH and Inhibin-B levels are seen in the patients. Up to 10 years of age, normal FSH and LH levels are seen. In mid to late puberty, there is a rise in the FSH and LH levels. There is a significant fall in testosterone and Inhibin-B levels. There will be an increase in the SHBG levels (sex hormone binding globulin). Increased Estradiol levels are seen in the patients, which is caused by the peripheral conversion of increased testosterone to estradiol.
- A testicular biopsy is conducted to arrive at the correct diagnosis. Before puberty, absent or reduced germinal cells can be seen. After puberty, the following features are seen: Hyalinized seminiferous tubules, Adenomatous clumps of Leydig cells, Predominance of sertoli cells, Azoospermia can lead to infertility in these males.
- Karyotype is considered to be the gold standard investigation. DEXA scan needs to be performed when bone mineral density is low in most patients. Fasting blood glucose, HbA1C, and lipid profile can be done post-puberty.
Management
- Testosterone therapy is the mainstay form of treatment. Preparation used is testosterone enanthate or cypionate. Starting dose is 25 to 50 mg intra-muscular injection every three to four weeks. Every 6 to 9 months, the dose was increased by 50 mg until a maintenance dose (200 to 250 milligrams every 3 to 4 weeks) for adults was achieved. For adults, testosterone patches or testosterone gel are also available as a form of management. Testosterone therapy will improve the secondary sexual characteristics, bone mineral density, and overall well-being of the patient. The area of cognition in the patient may also be improved. However, there is no effect on fertility. Gynecomastia needs to be managed by Aromatase inhibitors, but if these are not sufficient, plastic surgery needs to be performed and many of these patients. Counselling needs to be performed because the patient's low self-esteem and self-confidence have often been observed, and they may often resort to substance abuse. In case of reduced fertility, if sperm extraction is conducted, followed by intracytoplasmic injection, fertility is seen to increase. However, by the age of 16 to 18 years, most of these children have very few sperms available. Sperm banking has often been resorted to for this reason however, in a country like India, it has not been possible.
Also Read: Progeria- Pathogenesis, Clinical Features and Treatment
47, XYY Syndrome
- The incidence of such a condition is one in 800 males. The extra Y chromosome is due to the non-disjunction of the paternal chromosome in meiosis 2. These patients have a normal appearance, normal fertility and normal intelligence. Some may have learning disabilities or behavioural abnormalities (ADHD-like behaviour). In the 1960 and 1970s, some false research was conducted, and it was suggested that these patients were criminals. This is not true because criminal behaviour depends on various factors like the environment in which the child is brought up, the upbringing, child abuse, violence at home, and also inherent sociopathic and criminal activities.
Also Read: KEY POINTS AND RECOMMENDATIONS IN PEDIATRIC ADVANCED LIFE SUPPORT
Hope you found this blog helpful for your NEET SS General Pediatrics preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Turner Syndrome
Incidence And Cytogenetics
Clinical Features
Adults And Children
Gonadal Dysgenesis
Increase Risks
Management Of Turner Syndrome
Antenatal Diagnosis Of Turner Syndrome
Q1. What are the most consistent features of Turner Syndrome?
Q2. Which variety of Turner syndrome is associated with low IQ?
Q3. Before 12 years of age, no estrogen or progesterone should be given.
Differential Diagnosis Of Turner Syndrome: Noonan Syndrome
Klinefelter Syndrome
Cytogenetics
Prevalence Of Klinefelter Syndrome
Clinical Features
Increased Risks Associated With This Syndrome
Investigations
Management
47, XYY Syndrome
Top searching words
The most popular search terms used by aspirants
- NEET SS Pediatrics
- NEET SS Pediatrics Important Topics
PrepLadder 4.0 for NEET SS
Avail 24-Hr Free Trial