Kawasaki Disease : History, Symptoms, Causes and Treatment
Oct 27, 2023

- Kawasaki disease is based on the name of Prof. Tomisaku Kawasaki (1925 – 2020). Another name for Kawasaki disease is acute mucocutaneous lymph node syndrome of childhood and Infantile PAN. (Not in use now). An acute, multisystem febrile illness is affecting medium-sized arteries. It is the 2nd most common vasculitis in the world. Most common vasculitis in the world. A most common cause of acquired heart disease in children in developed countries. Most common serious vasculitis in children.
Also Read: Aneuploidies Including Turner And Klinefelter Syndrome
Kawasaki Disease Cause
The exact cause of the disease is unknown. Sex: It is more common in males than in females. Age: It mostly occurs in young children. It is never seen in adults . 80% of children below 5 years of age are affected. The Peak age at which the disease is more common is 18-24 months. High risk is seen in Asians, especially in Japanese. The genes implicated are: ITPKC (A T cell regulator), CASP-3, BLK, FCGR2A. Single nucleotide polymorphism (SNPs) in HLA class 2 antigen. Mutations in the ITPKC gene cause Kawasaki disease; these children have a high risk of coronary artery aneurysms and resistance to therapy. Anti-endothelial cell antibodies are found to be increased in some children with Kawasaki disease
Pathology
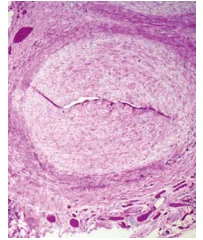
- Histopathology shows 3 phases: 1st phase: Neutrophilic necrotizing arteritis. 2nd phase: subacute/chronic arteritis. 3rd phase: Myofibroblast proliferates, which causes stenosis / obstruction.
Kawasaki Disease Symptoms
- Mnemonic: “FACE CREAM”. F - FEVER- High grade, remittent, lasts for > 5 days, unresponsive to antibiotics. C - CONJUNCTIVITIS- Bilateral, non-purulent. R - RASH - Polymorphous, does not have vesicles, bullae, or ulcerative lesions on the skin. E -EXTREMITIES- Acute changes lead to manifestations like edema and erythema of fingers/toes. Whereas subacute changes lead to desquamation of tips of fingers and toes. A - ADENOPATHY- Cervical lymphadenopathy, size >1.5 cm, unilateral. M - MUCOSAL - Oral and tongue regions are affected, but the classic feature is "Strawberry tongue." The tongue is swollen hypertrophied papillae and red. Other clinical features include gallbladder hydrops, perianal desquamation, beau's lines on the nail, irritability, joint pains. The latest clinical manifestation is Desquamation.
Also Read: The Genetics of Down Syndrome
Diagnosis Of Kawasaki Disease
- Kawasaki disease is diagnosed when there are symptoms like fever and any 4 out of 5 criteria (CREAM). Incomplete Kawasaki Disease: When there is fever, and only 2 or 3 criteria are fulfilled. Atypical Kawasaki: When there is fever and unusual/atypical organ failure, e.g., renal involvement. Fever + 3 criteria + echocardiography shows any cardiac abnormality. The patient is treated for Kawasaki disease.
.png)
Oral Mucosal Changes In Kawasaki Disease
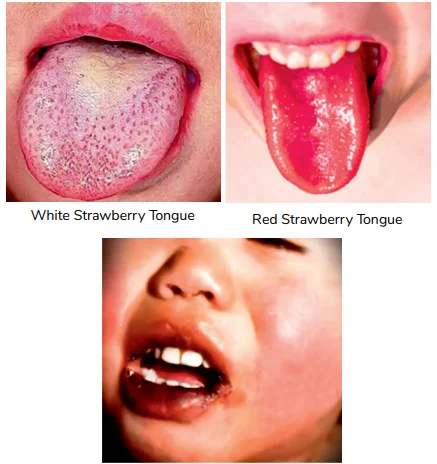
- Two types of tongue are described in the Kawasaki Disease: White strawberry tongue, Red Strawberry tongue. When not specifically mentioned, it refers to red strawberry tongue. White strawberry tongue: Tongue has a white coating, exudates are covering the surface of the tongue, hypertrophic papillae which are pink coloured are projecting out of the surface of the white coating. Is seen in the early stages of Kawasaki Disease, also seen in patients with scarlet fever. Red strawberry tongue more commonly seen in: Kawasaki Disease. White strawberry Tongue more commonly seen in: Scarlet Fever. Red Strawberry tongue is also seen in case of Scarlet Fever.
Bilateral, Non-purulent Conjunctivitis
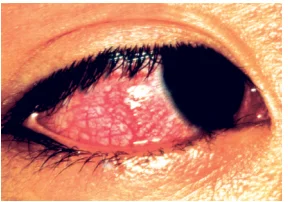
- Intense inflammation in the eyes without any puss discharge. A term which is also used for this condition is “Conjunctival Injection”
Natural History Of Kawasaki Disease
- ACUTE PHASE- Lasts 1 to 2 week, fever and other signs. SUBACUTE PHASE- lasts around 3 weeks, desquamation, increased platelet count., coronary artery aneurysm, most dangerous phase. CONVALESCENT PHASE- Occurs 6 to 8 weeks after onset, fever resolves, ESR normalizes.
New markers in Kawasaki disease
- Serum procalcitonin- It is average in Kawasaki disease but elevated in risk of coronary aneurysms. It is normally normal in Kawasaki Disease. Serum pro-BNP and serum NT-BNP- Helpful to differentiate from infection.
Also Read : Pigmentary Disorders in Children
Investigations
- Increased ESR , increased CRP- SENSITIVE TO MONITOR DISEASE ACTIVITY, increased neutrophils. Platelet count is normal or Increased in the subacute phase. Subacute face normalizes in 6 weeks. Thrombocytopenia is usually not seen in Kawasaki disease normally. If it occurs, if there is a high risk of coronary artery aneurysm, and it becomes resistant to treatment.
Complications
- The most common cardiac complication is myocarditis, seen in 50 - 70%, and can be asymptomatic. 2nd most common is coronary artery aneurysms: Seen in the subacute phase. If Kawasaki is untreated, the risk of CAA Is 20-25%. If left untreated, this can also lead to death. The cause of death can be thrombosis (most common cause), obstruction, and rupture. Kawasaki disease shock syndrome- Mitral regurgitation. Increased risk of asymptomatic pericardial effusion. Kawasaki disease can have atypical complications such as aseptic arthritis, aseptic meningitis, and macrophage activation syndrome.
Kawasaki Disease Treatment
- The drug of choice is: IVIG - A single dose of 2g/kg is given, Infusion is done over 12 hrs. Give within 7-10 days of onset. It can be useful even in presentations beyond 10 days if the patient has high ESR, CRP, and CAA. REGIMEN - IVIG (Single dose, once) + DAILY ASPIRIN (high dose) (50 mg/kg/day) high dose is given till the patient is afebrile for more than 48 hours. Then aspirin is shifted to a low dose (3-5/mg/kg/day) and given for 6 to 8 weeks, and then echocardiography is done. If the results are normal, then aspirin doses are stopped. If the findings are in resolving conditions, the aspirin is continued for 1 year. If the conditions are persistent, then anticoagulation treatment is considered.
IVIG- Resistant KD And its Management
IVIG Resistant KD
- When fever persists more than 36 hrs after IVIG infusion is completed. Seen in 15% cases. High risk of CAAs
Treatment
- Repeat the dose of IVIG and oral prednisolone(2g/day). If there is no response, consider anti-TNF alpha agents (infliximab). After that, consider cyclosporine and plasma exchange.
Differential Diagnosis
- If there is no fever or mild fever, the differential diagnosis of Kawasaki disease is Steven Johnson syndrome and toxic epidermal necrolysis. Another one is scarlet fever. Fever less than 5 days, responds to antibiotics. Tender lymphadenopathy which can be bilateral or unilateral pharyngitis. Evidence of streptococcal infection . Little to no cardiac manifestations. This can be used to distinguish scarlet fever over Kawasaki disease.
Also Read: Progeria- Pathogenesis, Clinical Features and Treatment
Clinical Questions
Q: what happens to fever if you do not give IVIG?
A: If untreated, fever continues for 1-3 weeks and resolves spontaneously by 3-4 weeks, the mean duration of fever being 11 days.
Q: What are the most common manifestations of Kawasaki disease?
A: Fever
Q: What is the least common manifestation of Kawasaki disease?
A: Cervical lymphadenopathy.
HIGH YIELD CONCEPT

Macrophage activation syndrome can develop in Kawasaki disease as a rare complication. How will you suspect and confirm? In severe Kawasaki disease, there is increased ESR and CRP. Whereas in Kawasaki with macrophage activation syndrome, ESR is normal to increase slightly, and CRP is increased. A useful marker is serum ferritin which is elevated in macrophage activation syndrome and is normal in Kawasaki disease.
Also Read: KEY POINTS AND RECOMMENDATIONS IN PEDIATRIC ADVANCED LIFE SUPPORT
Hope you found this blog helpful for your NEET SS General Pediatrics preparation. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
Kawasaki Disease Cause
Pathology
Kawasaki Disease Symptoms
Diagnosis Of Kawasaki Disease
Oral Mucosal Changes In Kawasaki Disease
Bilateral, Non-purulent Conjunctivitis
Natural History Of Kawasaki Disease
New markers in Kawasaki disease
Investigations
Complications
Kawasaki Disease Treatment
IVIG- Resistant KD And its Management
IVIG Resistant KD
Treatment
Differential Diagnosis
Clinical Questions
Top searching words
The most popular search terms used by aspirants
- NEET SS Pediatrics
- NEET SS Pediatrics Important Topics