Epilepsy AND Electroencephalography (EEG)
Apr 12, 2023

Epilepsy is a neurological disorder characterized by recurrent seizures, which can have a significant impact on an individual's quality of life. And, electroencephalography (EEG) is the diagnostic test that is commonly used to diagnose and monitor epilepsy. Understanding the clinical features, diagnostic workup, and management of epilepsy and EEG is essential for medical students.
In the NEET PG exam, there are often questions related to epilepsy and EEG, including the clinical features of different types of seizures, the indications and interpretation of EEG, and the management of epilepsy. Therefore, having a good understanding of epilepsy and EEG is crucial for success in the NEET PG exam.
Read this blog for a quick overview of this if important medicine topic for NEET PG exam preparation.
EEG

EEG is invented by Hans Berger and it has 10 – 20 lead placement system
- Alpha waves: seen when eyes are closed, drowsy, relaxed → 8 – 13 Hz
- Beta waves: when person is awake Awake, eyes opened → 13 - 30 Hz
- ϒ waves - 30-100 Hz(problem solving)
NREM Phase
- NREM 1 → Myoclonic jerk may occur.
- Theta waves: 4- 7 Hz are seen
- Theta waves: 4- 7 Hz are seen
- NREM 2 → longest phase of NREM
- µ waves/ sleep spindles are present
- 12 - 14 Hz
- NREM 3 → deepest phase of sleep/ most difficult to arouse
- Delta waves: 0.5 – 4 Hz are seen
Slowest wave pattern
- Maximum amplitude, least frequency
REM Phase
- REM sleep: Decreased tone of muscles is seen
- EEG shows Saw tooth pattern
Seizures
- Abnormal focus in the brain leading to abnormal electrical discharge.
Convulsion
- Motor manifestation of the same is called convulsion.

GTCS [Generalized Tonic Clonic Seizures]
Clinical Scenario
- Premonitory symptoms (general unwellness of the patient) are present
- later on loss of consciousness, up rolling of the eye balls and during tonus there is ↑ in Tone of muscles & sudden contraction of muscles of expiration of vocal cord occurs, which lead to “Ictal Cry”.
→ Up rolling of eyes
Tonus → Pooling of secretions
(10-20 → Tongue bite +
Seconds) → Perioral cyanosis
→ ↑ HR, ↑ BP
→ Mydriasis
- GCSE: Convulsions > 5 min
Clonus
- Violent jerking of all limbs followed by post ictal deficit
- Usual duration of both tonus and clonus: < 60 seconds
- Postictal deficit - confusion, loss of orientation
- Babinski sign is present and corneal reflex is absent in unconscious patients and vice versa at the time of regaining consciousness.
- Epilepsy: If > 2 unprovoked seizures episodes are seen it is k/a Epilepsy
| IMPORTANT INFORMATION To terminate Convulsion, Lorazepam is given intravenously. In case of failure to obtain intravenous access, rectal diazepam is used. |
Classification
|
Focal |
Generalized |
Unknown onset |
|
With intact awareness |
Motor
|
Motor |
|
Without intact awareness
|
Non – motor
|
Non – motor |
|
Unclassified |
- Aura implies perception of stimulus like bright lights, unpleasant smell of burning rubber
Focal Seizures
Causes
- Neurocysticercosis
- Hippocampal Sclerosis – causes temporal lobe epilepsy
With Intact Awareness
- Abnormal electrical activity in left motor cortex is seen
- Right hand/face involuntary movements are seen
| IMPORTANT INFORMATION Jacksonian march: Abnormal movement starts from distal part and progresses to proximal part. Todd’s palsy: Weakness persisting for hours to days after manifestation of focal seizures Epilepsia partialis continua: Counterpart of GCSE and manifestation can persist for days & weeks. |
Non Motor Manifestation
- Paresthesia / vertigo is seen
- Sensation of burning rubber
- Micropsia or macropsia
- Subjective events that cannot be observed by someone
- AURA like bright lights, the smell of burning rubber etc.
Also Read: Neurocysticercosis : Clinical Picture, Diagnosis, Treatment
Focal Seizure Without Intact Awareness
- AURA is not a feature of GTCS (generalized tonic clonic seizures). It is a feature of focal seizure
- Automatism
- It is a feature of focal seizure with impaired awareness
- Includes
- Lip-smacking
- Chewing
- Swallowing
- Picking
- Uncontrollable laughter/ crying
- Progression of focal seizure: AURA → Motionless stare → Automatism
- There is presence of
- Post ictal confusion
- Anterograde amnesia
- Transient neurological deficit in form of Aphasia
- EEG can be normal during interictal period
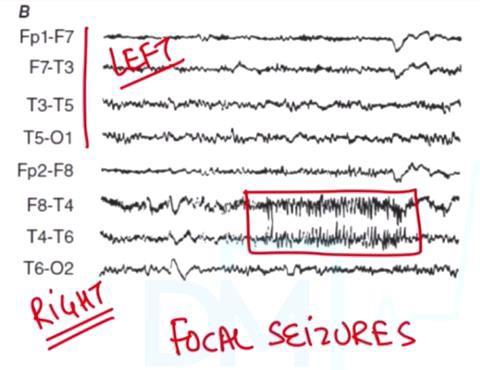
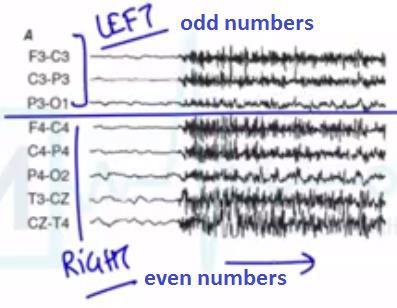
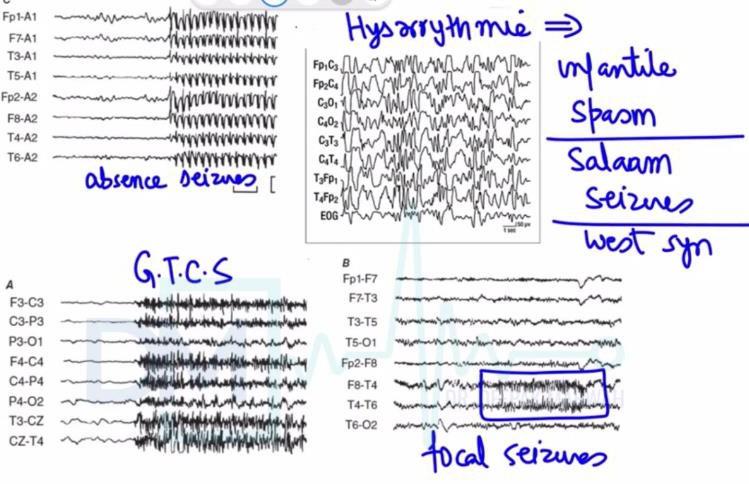
- The above EEG is showing Focal Seizures; possibly origin is from temporal lobe
Generalized Onset Seizures
- Typical absence seizures
- Transient loss of consciousness for 1-2 seconds
- Seen in 4-10 yr child
- Postural tone is maintained
- Become unresponsive/quiet
- Repeated blinking of eye is seen
- Post ictal deficit is absent
- Aka Day dreamers
- Vacate stare spell is seen
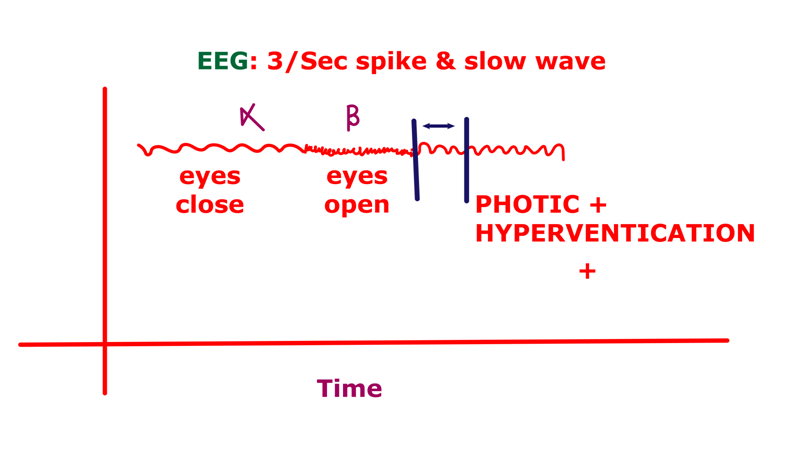
- EEG shows 3 per second spike & slow wave.
- Ask the patient to first open the eye – alpha wave present, then close the eye – beta wave present. Ask the patient to hyperventilate or give a photic trigger resulting in 3 per second spike & slow wave.
- T/t: Valproate/ ethosuximide (in younger child)
2. Atypical absence seizures
- EEG < 2.5 Hz spike by slow wave pattern.
- Lapse of consciousness is seen
- Mental retardation is seen
- Lennox gestaut syndrome
- Atonic seizures
- Loss of postural control for 1-2 sec
- Loss of consciousness for 1-2 sec
- Sudden onset of head nodding/dropping
| IMPORTANT INFORMATION Post ictal deficit is absent in Febrile seizure Absence seizure Atonic seizure |
- Myoclonic seizures
- Sudden/brief myoclonic jerky movements
- Causes
- Neurodegenerative disorder-Variant Creutzfeldt-Jakob disease
- Metabolic encephalopathy
- Anoxic cerebral injury - High altitude cerebral edema
- Epileptic spasm
- Infant with “SALAAM SEIZURES” involving trunk muscle
- On EEG: Hypsarrhythmia/ Grossly chaotic pattern is seen
- Background rhythm is suppressed (REM, NREM waves suppressed): Decremental response
- GTCS
- Premonitory symptoms
- Ictal cry: Tonus ~ 10 seconds
- Cyanosis, tongue bite +, up rolling eyes
- Clonus: involuntary jerking
- Post ictal deficit, Noisy breathing due to pooling of secretions
- Urine passed
- Stool passed
- Reorientation
Vasovagal Syncope Vs. GTCS
Vasovagal syncope GTCS Trigger Present None Tonus & clonus <15 seconds 30 – 60 seconds Tongue bite Rarely seen + Headache Rarely seen + Urinary incontinence + + Loss of consciousness Gradual Sudden Recovery Within seconds,
↑leg raiseMinutes to hours S. prolactin Normal ↑↑
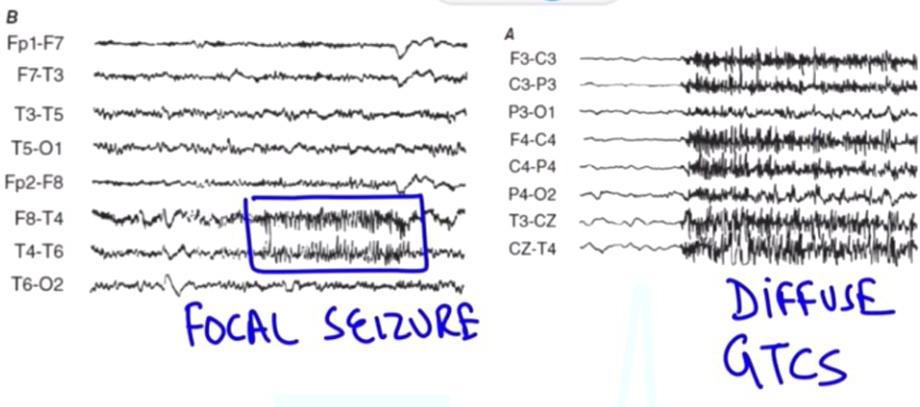
EEG of Focal seizure and Diffuse GTCS
Medicine Related Articles:
Epilepsy Syndromes
- Lennox Gastaut Syndrome
- GTCS
- Atypical absence
- Atonic seizure
- Etiology: multifactorial
- EEG shows <2.5 Hz spike & slow wave
- D.O.C: Na valproate
- JANZ syndrome/ Juvenile myoclonic epilepsy
- Polygenetic inheritance
- MC seen in 10 -19 yrs of age.
- Myoclonic Jerks (early morning) are seen
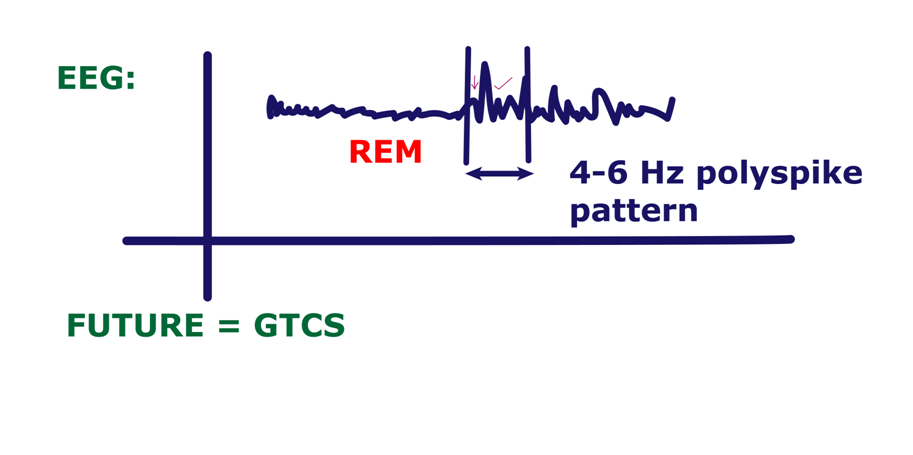
- EEG: 4-6 Hz Poly-spike patterns are seen.
- May develop GTCS in future and in 30% will also develop absence seizure in future
- Rx – Valproate (lifelong)
| IMPORTANT INFORMATION MYOCLONUS<1 yr: Infantile spasm/ Salaam seizure, WEST syndrome8 yr: Unvaccinated child; (measles vaccine not given) - Subacute sclerosing panencephalitis10-19 yr: Juvenile myoclonic epilepsy30 yr: Consumed Beef: Myoclonic JERKS + Dementia- Variant Creutzfeldt Jakob disease |
- Infantile spasm = hypsarrhythmia
- Juvenile myoclonic epilepsy = 4-6 Hz Polyspike pattern
- Mesial temporal lobe epilepsy
- MRI shows Hippocampal sclerosis
- Febrile convulsion
- Focal seizures with impaired awareness
- “Automatism” is seen
- EEG - temporal (U/L or B/L) spikes
- D.O.C: Sodium valproate
- T.O.C: Surgery- Surgical resection of hippocampal sclerosis lesion
Treatment
- Focal seizure = Carbamazepine
- Levetiracetam → elderly pt. (less interaction with other drugs)
- Lamotrigine → Steven Johnson syndrome risk
- Carbamazepine → Risk factor- anemia, leucopenia and hepatotoxicity
- Oxcarbazepine
- Phenytoin
| HOW TO REMEMBER L2COP |
- Generalized seizures DOC is Sodium valproate
- Safest Antiepileptic drug in pregnancy: Levetiracetam (Least teratogenic) > Lamotrigine
| GTCS | Focal seizure | Typical absence | Atypical absenceAtonic/ myoclonic |
| Lamotrigine Valproate Levetiracetam | Lamotrigine Levetiracetam Carbamazepine Oxcarbazepine Phenytoin | Valproate Lamotrigine Ethosuximide | Valproate Lamotrigine Topiramate |
Infantile Spasms
- D.O.C is ACTH
- D.O.C of infantile spasm with Tuberous sclerosis (Neurocutaneous disorder): Vigabatrin
| Previous year questions? Q. Choose the correct answer for juvenile myoclonic epilepsy? (AIIMS Nov 2019) A. Valproate is contraindicated B. Lamotrigine can be given C. Only use of benzodiazepines can cure JMED. Polygenic inheritance |
Febrile Seizures
- Prophylaxis: Oral clobazam
- T/t: intranasal midazolam/ Rectal Diazepam (conventional method)
- Most common epilepsy in children: Benign Rolandic epilepsy
- Episodes of Focal seizures is seen
- Peak age of onset: 2-13 yr
- Treatment: Carbamazepine
- MC seizures in child: Febrile seizures
- Mc seizures in neonate: Subtle seizures
‘Jitteriness’ Causes: Hypoxic ischemic encephalopathy and Hypoglycemia
EEG
Summary Table
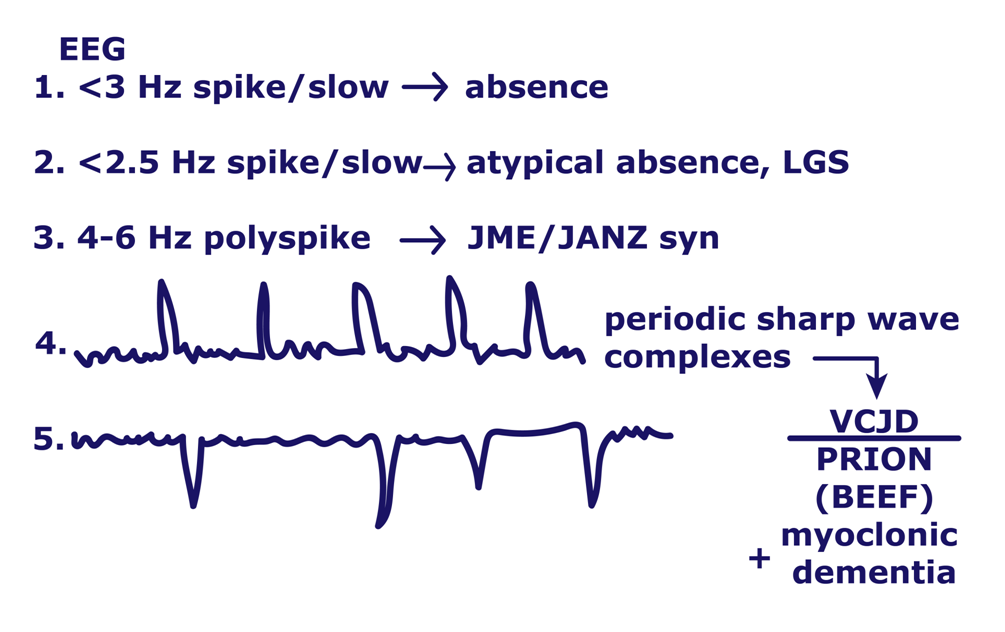
| < 3 Hz spike / slow: Absence seizures < 2.5 Hz spike/ slow: Atypical Absence seizures 4-6 Hz Polyspike: Juvenile myoclonic epilepsy Periodic sharp wave complexes : VCJD Triphasic waves: seen in Hepatic encephalopathy |
.jpg)
Subacute Sclerosing Panencephalitis
- Also called as Slow virus disease
- It is late complication of measles
- On EEG – Periodic sharp wave complex is seen
- 2 yr: Measles Vaccine is not given
- 8 yr: C/F are
- Myoclonic jerk
- Neurodegeneration features – Apathy
- Urinary incontinence
- Stool incontinence
Diagnosis
| Clinical | Progressive, subacute metal deterioration with typical signs like myoclonus |
| EEG | Periodic, stereotyped, high voltage discharges |
| Cerebrospinal fluid | Raised gamma globulin or oligoclonal pattern |
| Measles antibodies | RAISED Titre in serum (≥ 1:256) and /or cerebrospinal fluid (≥ 1:4) |
| Brain biopsy | Suggestive of pan encephalitis |
| Definitive: criteria 5 with three more criteria; probable: three of the five criteria. | |
Also Read :
Cardiopulmonary Resuscitation: How to Perform CPR, Types of CPR
Biomedical Waste Management: Types, Different Coloured Bins For BMW And Treatment Methods
Phakomatosis/ Neurocutaneous Disorder
Tuberous sclerosis: AD
- Family history is present
- TSC1 (Chromosome 9) & TSC2 gene (Chromosome 16) involvement is seen
 |    |
- Adenoma sebaceum- Acne like lesion in butterfly distribution is seen
- Shagreen patch: Irregular appearance of skin is seen
- Subungual fibroma: fleshy growth from below the nail is seen
Earliest Cutaneous Manifestation
- Ash- leaf macules: Hypopigmented macules on Trunk
CNS Manifestations
- < 1yr: Infantile spasm = Vigabatrin
- > 1 yr : Focal/ seizures = Carbamazepine
- On CT, Subependymal astrocytoma is seen
- Lesion in Kidney: Angiomyolipoma (having fat, muscle and blood vessel together)
- Bleeding in angiomyolipoma of Tuberous sclerosis is k/a Wunderlich syndrome
Sturge Weber Syndrome
- Port wine stain
- Cavernous angioma
- Seizures (focal)
C/F
- S – Seizure
- T – Trigeminal Nerve distribution
- U – U/L weakness
- R – Mental Retardation
- G – Glaucoma
- E - Eye = Buphthalmos
CT scan head shows Tram Track Appearance
| HOW TO REMEMBER STURGE |
| IMPORTANT INFORMATION TRAM TRACK APPEARANCE on CT scan head : Sturge weber syndrome Chest X-ray : BRONCHIECTASIS kidney Biopsy: MPGN |
Study medicine from experts. Download the PrepLadder app and get access to high-quality learning resources including video lectures, study notes and MCQs for practice.

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
GTCS [Generalized Tonic Clonic Seizures]
Clinical Scenario
Classification
Focal Seizures
Non Motor Manifestation
Focal Seizure Without Intact Awareness
Generalized Onset Seizures
Vasovagal Syncope Vs. GTCS
Epilepsy Syndromes
Treatment
Infantile Spasms
Febrile Seizures
Subacute Sclerosing Panencephalitis
Phakomatosis/ Neurocutaneous Disorder
Tuberous sclerosis: AD
Earliest Cutaneous Manifestation
Sturge Weber Syndrome
Top searching words
The most popular search terms used by aspirants
- NEET PG Medicine
- NEET PG Strategy