20 Must-Know Obstetrics And Gynaecology Flashcards NEET PG 2026
Feb 26, 2026

FLASHCARD 1
Ovulation
Ovulation of the follicle around the 14th day of the menstrual cycle
↓
Oocytes will be released into the fallopian tube.
↓
Shrinkage of the follicle forms the corpus luteum (Yellow color body)
↓
The Corpus luteum will produce progesterone.
↓
Progesterone will make the endometrial glands secretory.
↓
Fertilization will occur at the site of the ampulla.
↓
The embryo will reach the uterine cavity on the 3rd to 4th day.
↓
Implantation occurs on the 6th day after ovulation or fertilization – earliest
↓
It can also occur from the 6th to the 10th day of ovulation (20 to 24 days of the menstrual cycle)
Follicular Stimulating Hormone
- Normal level: 2 to 6 IU
- Purpose: Produce Estrogen
- Suggestive of menopause: >10 IU
- Diagnostic of menopause: >40 IU
- Premature ovarian failure: FSH >40 IU in <40 years
FLASHCARD 2
Menstrual Cycle Chart
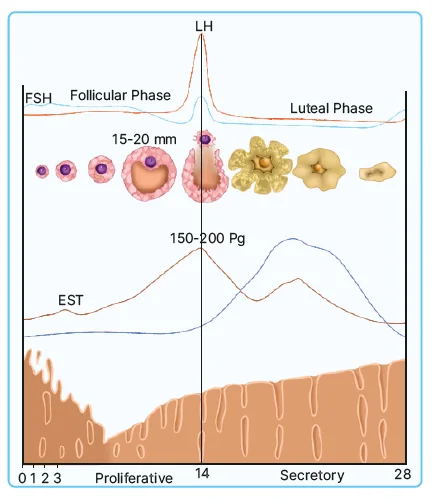
- Cycle starts with bleeding – Day 1
- Initially, FSH is high, decreases in mid, and again increases at last
- Heartbeat of infant: 5 weeks and 3 days
- FSH: Recruit 7 or 8 Antral follicles
- Low FSH will maintain the growth of one follicle (Size 15 to 20 mm)
- Estrogen levels will be increased (150 to 200 pg)
- So it is known as the proliferative phase
- Other Name: Follicular Phase
- LH surge will occur as the estrogen gives singles to the brain
- The follicle will shrink and become the corpus luteum
- The corpus luteum will produce progesterone
- The size of the glands is not increased
- Hence, it is known as the secretory phase
- Other Name: Luteal Phase
- The corpus luteum also secretes some amount of estrogen
- The corpus luteum reduces in function by day 24 and is lost by day 28.
- That endometrium will degenerate and shed.
|
|
Menstrual Cycle: Of Sexually Active Women
Implantation of the embryo will occur on the 6th day after ovulation or fertilization
↓
The embryo is implanted in the secretory endometrium
↓
The corpus luteum will work only for 10 days
↓
Early cells of the placenta: Syncytiotrophoblasts will produce the HCG
↓
Human chorionic gonadotropin will protect the corpus luteum from degeneration
↓
It helps to maintain the pregnancy
FLASHCARD 3
Progesterone Challenge Test

FLASHCARD 4
Sonographic Criteria for PCOS

- It has no cyst
- Enlarged ovary with a chain of small follicles i.e. necklace of chain appearance.
- Shape: ring of pearl
- Presence of 20 or more Follicles in either ovary measuring 2 to 6 mm in diameter (Less than 9 mm): Antral size follicles
- Thick stroma
- Increased ovarian volume: >10 ml
- A single ovary meeting these criteria is sufficient to affix the PCOS morphology
Syndrome of PCOS
- Anovulation is associated with infertility
- Periods after 35 days: Oligomenorrhea
- Missing 3 regular cycles of menstruation: Amenorrhea
.jpg)
Quick Revision of PCOS

- FSH is very low
- Estrogen is increased
- Sends positive feedback to the brain
- As a result, LH levels will be increased
- Progesterone is low, no secretory action
- Proliferation occurs continuously
FLASHCARD 5
Symptoms of Ca Cervix
- Most common is post-coital or post-menopausal bleeding
- Pyrometra causing dirty, foul, smelling discharge
- Uremia: Most common cause of death

Staging of Ca Cervix

FLASHCARD 6
Ca Endometrium Staging

Ca Endometrium Management
- Rule out any local lesions
- After the physical examinations, and observe all the local lesions
- If there are no local lesions, 1st step is office endometrial biopsy using a pipelle
- Easy procedure
- 90% sensitive
- Fractional curettage (D&C)
- Assess all the fractions of the uterus
- 95-99% sensitive
- Hysteroscopy biopsy
- 100% sensitive
- Best method
- TVS: good adjunctive procedure
- In postmenopausal women, endometrium
- Common site of the recurrence of ca endometrium is : vault of the vagina
- 1st line treatment of recurrence is progesterone therapy
- Radiation is the best treatment for recurrence.
FLASHCARD 7
Dysgerminoma
- Most common germ cell malignancy: 40-45%
- Only bilateral germ cell malignancy in 10-15% of cases
- Large fleshy tumour
- Frequently associated with hypercalcemia
- 5% associated with dysgenic gonads
- Seminoma-type cells
- Large polygonal cells with clear cytoplasm and dark nucleoli and back-to-back arrangements
- Increases LDH, placental alkaline phosphatase, and even HCG, but not Alfa fetoprotein.
FLASHCARD 8
Adenomyosis

- It is referred to as endometriosis interna, endometriosis occurring within the muscle layer.
- Hysterectomy specimen examination
- Lakes of uterine blood are found in uterus muscles
- Hyperplasia of uterine muscle.

FLASHCARD 9
Staging of Prolapse based on POP-Q
Stage of Prolapse
Extent of prolapse in relation to hymen
Prolapse above the hymen: Negative Numbers
Prolapse below Hymen: Positive Numbers
Stage 0: No Prolapse
Stage I: The most distant portion of prolapse descends to a point less than 1cm above the hymen
Stage II: Maximum Descent is within 1 cm of Hymen
Stage III : Prolapse extends more than 1 cm beyond hymen but no more than 2 cm of Total Vaginal length
Stage IV : Complete eversion of vagina or descent within 2 cm of the vaginal length
FLASHCARD 10
Types of pills
Four generations: based on types of progesterone
- 1st generation · Norethindrone, lynestrenol, Norethisterone
- 2nd generation · Etonogestrel, Norgestrel
- 3rd generation · Desogestrel, Gestodene, Norgestodene
- 4th generation : Drosperinone (potent progestogenic-antimineralocorticoid- anti androgenic)
Protocol for Starting the Pills
- Regular cycles: 1st to 5th day of periods
- Breastfeeding: After 6 months of Exclusive B.F.
- After delivery & not breastfeeding: After 4 weeks of delivery
- Post-abortion: From immediately to 7 days after
- After Emergency Contraception: Same Day! Don't have to wait for the next period!
Emergency Contraception
- If women doesn't want to have children: Combined oral contraceptive pill/IUCD
- If women have children, are pregnant, and don't want children anymore: Medical termination of pregnancy.
- If a woman had intercourse and has not taken contraception, where she is too early for abortion: Interception of a pregnancy (Emergency contraception) within 72 hours of unprotected intercourse.
FLASHCARD 11
Male Sterilization : Non-Scalpel Vasectomy (NSV)

- Tools
- Anesthesia is given, and a 1-stab incision is given
- A stab incision is created by the sharp artery forceps
- Stabilizing the Vas by ring forceps
- Babcock's forceps are used for tubal ligation in females
- Can be done in 5-7 minutes
- A simpler procedure
- After the vasectomy, the man is not sterile until the path is not emptied of sperm (3 months or 20 ejaculates)
- Later, semen analysis is done (Azoospermia)
- Safe procedure
FLASHCARD 12
ESHRE Classification of Mullerian Defects

FLASHCARD 13
Hypertension in Pregnancy

FLASHCARD 14
Treatment of Gestational Hypertension and Pre-Eclampsia
- Labetalol: DOC ( can be given up to 2400 mg/24hrs)
- Methyldopa: Previous drug of choice, a prodrug 250-500mg QID
- Nifedipine: 5-10 mg TID upto 80 mg/24hrs
- Prazosin: 2.5mg OD or BD
- Hydralazine: 25mg per day
- Contraindicated Drugs:
- ACE Inhibitors:
- Hypocalvaria
- Renal agenesis
- Oligoamnios
- β - Blockers
- Frusemide
- All the above three drugs are known to cause IUGR.
- ACE Inhibitors:
FLASHCARD 15
Problems with Diabetes in Pregnancy
|
Maternal |
Neonatal Problems |
|
|
FLASHCARD 16
Treatment of abortion: 1st trimester
Dual marker at 12 weeks:
- PAPP-A - pregnancy-associated plasma protein A reduces
- HCG - increases
NT NB scan at 12 weeks
- Nuchal translucency > 3 mm - increased risk
- Absent nasal bone or short-increased risk
Triple marker at 16 weeks
- UE3 - unconjugated estriol reduced
- AFP - reduced
- HCG - increased
Quadruple marker at 16 weeks
- Triple + inhibin
- Inhibin high
FLASHCARD 17
Placenta Previa
- Incidence - 1 in 300-400 pregnancies
- Associated with
- Multiparity
- Twin gestation
- Large placenta
- Previous cesarean section
- Placenta accreta
- Previous hysterotomies, myomectomies

FLASHCARD 18
Causes of PPH Postpartum Hemorrhage
|
Abnormal Tone |
Trauma - injuries |
|
Any bleeding in the genital tract after delivery is called PPH |
|
Thrombin - Coagulation defects |
Tissue - Retained bits |
|
FLASHCARD 19
Uterine Devascularization

FLASHCARD 20
Overview of Physiological Change in Pregnancy


Download the PrepLadder app now and unlock a 24-hour FREE trial of premium high-yield content. Access Smarter Video Lectures also in हिंglish, Game Changing Qbank, Audio QBank, Structured Notes, Treasures, Mock test for FREE to ace your NEET PG preparation. Elevate your study experience and gear up for success. Start your journey with PrepLadder today!

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Navigate Quickly
FLASHCARD 1
Ovulation
Follicular Stimulating Hormone
FLASHCARD 2
Menstrual Cycle Chart
Menstrual Cycle: Of Sexually Active Women
FLASHCARD 3
Progesterone Challenge Test
FLASHCARD 4
Sonographic Criteria for PCOS
Syndrome of PCOS
Quick Revision of PCOS
FLASHCARD 5
Symptoms of Ca Cervix
Staging of Ca Cervix
FLASHCARD 6
Ca Endometrium Staging
Ca Endometrium Management
FLASHCARD 7
Dysgerminoma
FLASHCARD 8
Adenomyosis
FLASHCARD 9
Staging of Prolapse based on POP-Q
FLASHCARD 10
Types of pills
Protocol for Starting the Pills
Emergency Contraception
FLASHCARD 11
Male Sterilization : Non-Scalpel Vasectomy (NSV)
FLASHCARD 12
ESHRE Classification of Mullerian Defects
FLASHCARD 13
Hypertension in Pregnancy
FLASHCARD 14
Treatment of Gestational Hypertension and Pre-Eclampsia
FLASHCARD 15
Problems with Diabetes in Pregnancy
FLASHCARD 16
Treatment of abortion: 1st trimester
FLASHCARD 17
Placenta Previa
FLASHCARD 18
Causes of PPH Postpartum Hemorrhage
FLASHCARD 19
Uterine Devascularization
FLASHCARD 20
Overview of Physiological Change in Pregnancy
Top searching words
The most popular search terms used by aspirants
- NEET PG OBSGYN
- NEET PG OBSGYN Preparation
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial